


Dr. Johanna Olson-Kennedy's Pediatric Gender Clinic Is Shutting Down
Under pressure from all sides from the Trump administration, the gender clinic at Children's Hospital Los Angeles will shut its doors next month, the Los Angeles Times reports

The pediatric gender clinic led by Dr. Johanna Olson-Kennedy at Children’s Hospital Los Angeles will shut its doors next month, The Los Angeles Times reported today. Founded shortly after the so-called Dutch model of providing puberty blockers, cross-sex hormones and gender-transition surgeries to minors with gender dysphoria was first imported to Boston Children’s in 2007, the Center for Transyouth Health and Development at CHLA is one of the largest pediatric gender clinics in the nation. According to the Times, the hospital felt it could no longer withstand the pressures coming from all sides by the Trump administration, which from the outset has made it a mission to end gender-transition medical interventions among children.
The Times reports:
Under mounting pressure from the Trump administration, Children’s Hospital Los Angeles will shutter its longstanding healthcare program for trans children and young adults this summer, according to emails reviewed by The Times.
The Center for Transyouth Health and Development began telling its nearly 3,000 patient families of the closure on Thursday, saying there was “no viable alternative” that would allow the safety-net hospital to continue specialized care.
“There is no doubt that this is a painful and significant change to our organization and a challenge to CHLA’s mission, vision, and values,” hospital executives wrote to staff in a Thursday morning email.
The email said the decision to close the center on July 22 “follows a lengthy and thorough assessment of the increasingly severe impacts of federal administrative actions and proposed policies” that have emerged since the hospital briefly paused the initiation of care for some patients this winter.
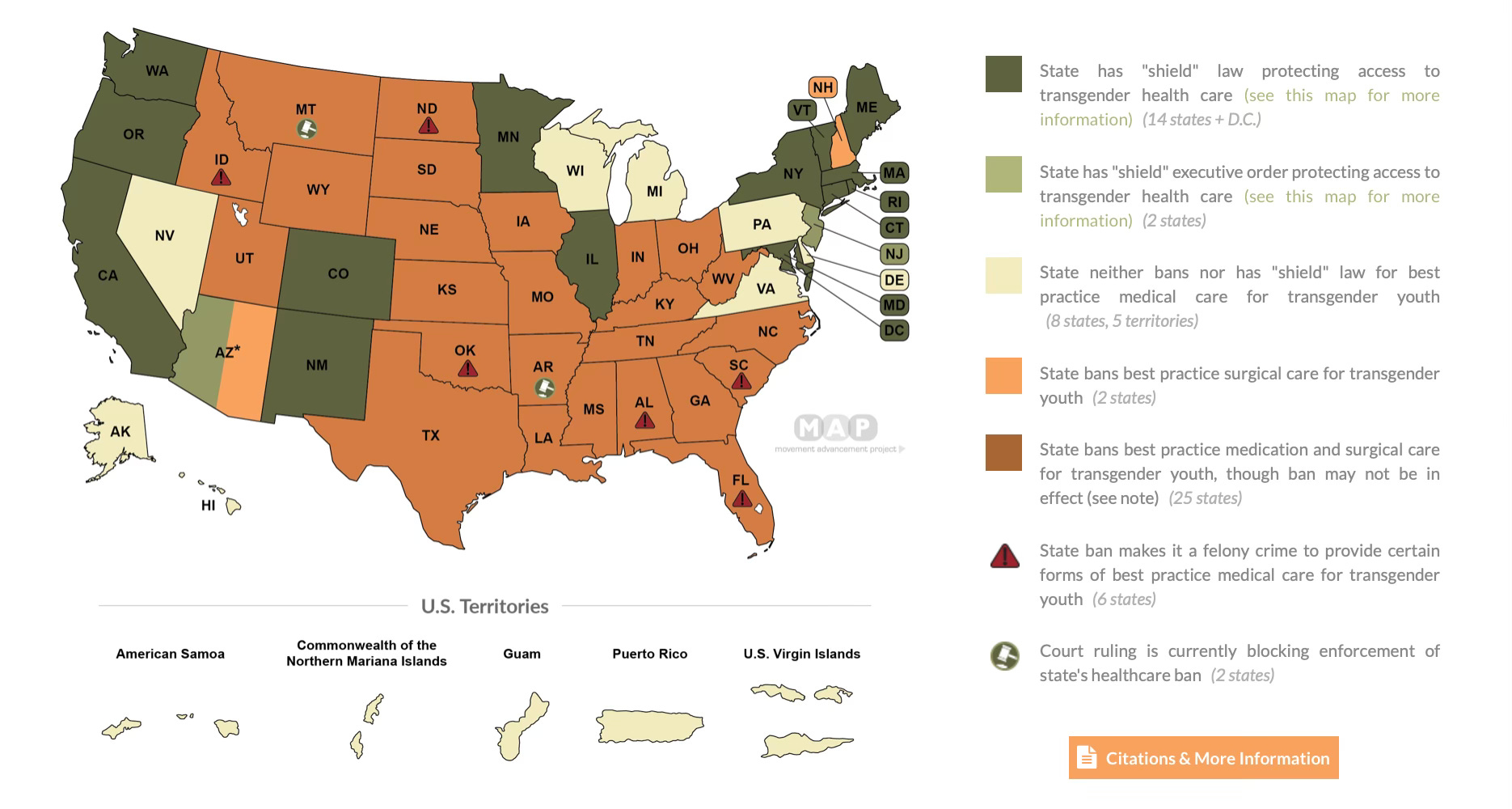
The fall of Dr. Olson-Kennedy’s clinic offers a chilling harbinger for the entire field of pediatric gender medicine in the United States. By the end of the month, the Supreme Court will decide the U.S. v Skrmetti case, which will determine whether Tennessee’s ban of pediatric gender-transition treatment violates the Equal Protection Clause of the 14th Amendment. If the court upholds the law, as it is widely expected to do, this will likely entrench bans of these treatments in 26 states (New Hampshire is on the verge of becoming the 26th state). But even if by some chance the law is overturned, the Trump administration has made the climate for providing these treatments so forbidding, we could still see the nation’s major clinics begin to fall like dominoes.
According to the Times, CHLA was particularly exposed because it receives so much of its revenue from Medicaid—a major point of leverage that the Trump administration apparently holds over hospitals as it seeks to strong-arm the end of these controversial medical practices.
First there was the executive order Trump issued in January, barring federal funding from supporting health care providers that provide gender-transition interventions to people under age 19. However, a federal judge in February issued a temporary restraining order against the order.
But during the months, since then:
Attorney General Pam Bondi has ordered prosecutors to investigate physicians who have provided gender-transition surgeries.
HHS Secretary Robert F. Kennedy Jr. issued a letter to care providers urging them to cease following WPATH’s Standards of Care 8 and instead to take guidance from the HHS report on pediatric gender medicine, which argued that these treatments are too risky to even be studied in clinical trials.
The FBI issued a call for tips on any providers providing these surgeries to children.
Last week, Dr. Olson-Kennedy was featured prominently in The New York Times’ six-part podcast series on pediatric gender medicine, The Protocol. The podcast described how she became the leading figure in a movement to ease the Dutch model’s rigid gatekeeping requirements and to establish a fully American, gender-affirming method in which the child’s wants, needs and self perception led the way in their care. Psychologist Laura Edwards-Leeper, who was part of the team that first imported the Dutch model to Boston Children’s, served as a foil for Dr. Olson-Kennedy in the podcast. Dr. Edwards-Leeper advocated for more careful, cautious, and drawn out psychological assessments of children before deciding whether they were good candidates for puberty blockers and cross-sex hormones.
Dr. Olson-Kennedy has long been outspoken about her support for open access to gender-transition drugs for children. In this interview with NBC’s Hoda Kotb, which seems to belong to another time (no mainstream journalist would dare express such skepticism today as Ms. Kotb does in the clip) Dr. Olson-Kennedy argued that children should receive these drugs, because absent them their suicide risk is so severe.
Only one study has ever directly assessed whether prescribing cross-sex hormones to youths attending gender clinics is associated with an independent, statistically significant difference in the suicide death rate. The study, an analysis of comprehensive, nationalized health data from Finland that was published last year, found no such association. It found that while elevated among youth who attend gender clinics, suicides were nevertheless rare, and that they were not independently associated with attending such a clinic, but with a high rate of attending specialist psychiatric appointments—a proxy for severe mental illness.
I remain perplexed that I was the only U.S. journalist to cover this important study for a major news outlet, the New York Post. I was criticized by the head of the US branch of WPATH for doing so. In a March 2024 letter to colleagues, Dr. Carl Streed wrote of the study, “I seriously question the motives and ethics of any reporter, legislator, or professional citing it as evidence.”
Dr. Edwards-Leeper told Times journalist Azeen Ghorayshi that she feared that what she saw as Dr. Olson-Kennedy’s reckless approach to caring for gender dysphoric children would lead to a backlash that would hurt the field as a whole.
It appears that Dr. Edwards-Leeper’s perspective was prescient. Unless, however, one believes that Republicans would have leveraged this medical field as a wedge issue to feed red meat to their base regardless of how carefully its leading providers carried out their efforts to care for the burgeoning population of gender dysphoric kids.
Last week, I reported on the long-awaited publication of the study on puberty blockers that Dr. Olson-Kennedy, according to reporting by Ms. Ghorayshi, withheld from publishing for political reasons. The study found that the children were largely psychologically well when they started puberty blockers, typically at the age of 11, but as young as eight years old, and that their mental health remained fairly stable for the year or two they spent on the drugs.


I previously started reporting a 12-part series of training videos that Dr. Olson-Kennedy, her social-worker husband, Dr. Aydin Olson-Kennedy, and their colleague provided last year to mental health providers on how to provide the gender-affirming care method. The series has now taken on the air of a time capsule of an approach to gender dysphoria treatment that would soon meet its demise—at least at CHLA.



And in December, I reported on the lawsuit waged against Dr. Olson-Kennedy by a former patient to whom she prescribed puberty blockers on the first visit, when the girl was 12, without providing any psychological assessment, and when the child had not yet been experiencing gender-related distress for long enough to even qualify for a gender dysphoria diagnosis. Dr. Olson-Kennedy put the child on testosterone at age 13 and signed off on her double mastectomy at age 14. The child ultimately detransitioned as a young adult and sued. Shortly after, she had surgery to reconstruct her breasts.

Dr. Olson-Kennedy is most known for saying in a different training session that was caught on tape, “What we do know is that adolescents actually have the capacity to make a reasoned, logical decision. And here’s the other thing about chest surgery: If you want breasts at a later point in your life, you can go and get them.”
As for Dr. Olson-Kennedy, if she is to continue to treating children and counseling them to have their breasts removed, she will have to go out and get a job at a different clinic. That is, if there are still pediatric gender clinics left who can employ her.
UPDATE: June 13, 4:30pm
Here is the full text of the email that CHLA leadership sent out explaining why they were shutting down the pediatric gender clinic:
Dear CHLA Team Members,
We are writing to share an important and profoundly difficult update. CHLA has determined that—under current conditions and despite significant efforts to avoid this outcome—there is no viable alternative to closing the Center for Transyouth Health and Development, along with the Gender-Affirming Care (GAC) surgical program. As a result, the Center and program will be closing, effective July 22, 2025.
This decision does not come lightly and we realize the deep impact it will have on members of our team and community, especially following the hospital’s decision to pause and then resume new enrollments to certain aspects of CHLA’s gender-affirming care services. However, it follows a lengthy and thorough assessment of the increasingly severe impacts of federal administrative actions and proposed policies that have taken place since that time, including recent developments that directly affect CHLA.
We are starting to notify patients today, and over the next several weeks CHLA care teams will be actively assisting with patient navigation and seeking to identify potential alternative providers. CHLA will explore reassigning impacted employees to other roles within the hospital based on needs and available funding.
Why Now
As we have shared, CHLA continues to face significant operational, legal, and financial risks stemming from the shifting policy landscape at both the state and federal levels. Over the past several months, California’s deepening budget crisis, President Trump’s executive orders, proposed federal legislation and rulemaking, and growing economic uncertainty have made the situation even more dire. Alone, each of these developments would pose a significant challenge to CHLA—together, they are creating an immediate and unsustainable strain on our fiscal resiliency, threatening our ability to serve the hundreds of thousands of patients who depend on CHLA for lifesaving care and to maintain scientific research that is so crucial to our mission.
In the end, this painful and difficult decision was driven by the need to safeguard CHLA’s ability to operate amid significant external pressures beyond our control. The July 22 sunset date was chosen to help give patient families adequate time to plan for moving care to providers less impacted by the legal and financial pressures our health system faces.
External Factors Impacting this Outcome
When the executive order impacting GAC was first issued, there was significant uncertainty about how the order would be interpreted and enforced. CHLA’s earlier decision to pause initiation of new hormonal therapies for patients seeking GAC (as well as surgeries for minors) reflected that uncertainty and how it would impact hospital operations. A few weeks later, CHLA was able to resume these therapies after reviewing temporary restraining orders on the executive order, and in light of commitments from the state Attorney General’s office to seek additional protections for CHLA and our patients.
However, more recently, federal agencies—including the Department of Justice (DOJ), Health and Human Services (HHS), Centers for Medicare and Medicaid Services (CMS), the FBI, and the Federal Trade Commission—have taken actions to clarify the executive order impacting GAC, including severe consequences for hospitals and other providers that do not comply.
These clarifications include messages sent directly to CHLA and/or disseminated nationally:
Letters dated May 28, 2025, from CMS and HHS demanding data on hospital quality standards and finances related to GAC within 30 days of receipt and warning of “new policies and oversight actions...to hold providers...accountable” if changes to care practices are not made to come into alignment with the new HHS review.
A memo from U.S. Attorney General Pam Bondi in late April directing DOJ attorneys to enforce the Administration’s executive order on GAC through federal criminal prosecutions of GAC providers; calling for False Claims Act investigations of GAC providers; and stating the DOJ was “eager” to work with whistleblowers to identify these providers.
An HHS review published in May dismissing current evidence-based care protocols and standards of care while promoting alternative best practices for the treatment of pediatric gender dysphoria, which included dozens of references to CHLA and the Center for Transyouth Health and Development.
Taken together, the Attorney General memo, HHS review, and the recent solicitation of tips from the FBI to report hospitals and providers of GAC strongly signal this Administration’s intent to take swift and decisive action, both criminal and civil, against any entity it views as being in violation of the executive order.
In addition, if CMS were to give CHLA an “Immediate Jeopardy” designation –– the highest level of deficiency identified by CMS –– in connection with its continued provision of GAC to minors, CHLA would be suspended or terminated from our ability to participate in Medicaid/Medi-Cal, posing an existential threat to our hospital operations.
These threats are no longer theoretical. The federal government has already cut off hundreds of millions of dollars from U.S. academic and research institutions for noncompliance with executive orders, often with little to no warning. Many of these organizations are also facing inquiries from agencies such as the DOJ and HHS.
Why CHLA
We understand that other hospitals may not yet be taking this step, and this may prompt questions about why CHLA is doing so. It’s important to share why CHLA’s ability to continue serving children and families across the region is uniquely tied to state and federal support:
CHLA relies on federal funding more than any other pediatric hospital in the state. Over 65% of our annual funding—$1.3 billion out of $2 billion—comes from federal sources. For the past several years, CHLA has faced increasing financial strain due to this reliance on government funding and a payer mix heavily weighted toward Medi-Cal, which has been steadily lowering reimbursement for care of California’s sickest children. This environment has contributed to CHLA's bond rating being downgraded to a level that is now below investment-grade, reflecting the hospital’s less stable financial position.
Should CHLA lose access to federal funding, the hospital’s cash reserves would only be able to sustain operations for approximately 50 days. Our fragile fiscal position, combined with our reliance on threatened federal funding, means CHLA is uniquely vulnerable to regulatory and policy changes impacting Medicaid participation and reimbursement. Long periods of uncertain reimbursement policy would threaten CHLA’s ability to remain open.
Threats to CHLA’s funding also directly threaten access to essential care for hundreds of thousands of Southern California children, adolescents, and young adults, who are disproportionately low-income and underserved. As the largest pediatric safety net provider in California, CHLA accounts for nearly 40% of pediatric beds in LA County. We fully recognize that this decision will have a real impact on a population that is itself vulnerable, which makes this outcome all the more heart-wrenching. But CHLA has a responsibility to navigate this complex and uncertain regulatory environment in a way that allows us to remain open as much as possible for as many as possible.
Again, there is no doubt that this is a painful and significant change to our organization and a challenge to CHLA’s mission, vision, and values. Our colleagues, both within and outside of the Center for Transyouth Health and Development and the Division of Adolescent and Young Adult Medicine, are passionately committed to caring for youth, and we expect many other team members will also have a range of emotions and reactions that to this decision and the moment in which it is being made. For more than 30 years, CHLA has provided this high-quality, evidence-based, medically essential care for youth, young adults, and their families. CHLA is immensely proud of this legacy of caring for young people on the path to achieving their authentic selves. Despite this deeply held commitment to supporting LA’s gender-diverse community, the hospital has been left with no viable path forward.
We understand that this news will be surprising and unwelcome for many, and that you may have additional questions. We will be hosting a series of team member forums over the next few days to hear your thoughts and concerns while addressing some of your questions.
Sincerely,
PAUL S. VIVIANO
Chief Executive Officer
KELLY M. JOHNSON, PhD, RN, NEA-BC
Senior Vice President and Chief Nursing Officer
LARA KHOURI
President and Chief Operating Officer
MARK D. KRIEGER, MD
Senior Vice President and Surgeon-in-Chief
JAMES STEIN, MD, MSc, FACS, FAAP
Senior Vice President and Chief Medical Officer
ALAN S. WAYNE, MD
Senior Vice President and Pediatrician-in-Chief
I am an independent journalist, specializing in science and health care coverage. I contribute to The New York Times, The Guardian, NBC News and The New York Sun. I have also written for theWashington Post, The Atlantic and The Nation. Follow me on Twitter: @benryanwriter and Bluesky: @benryanwriter.bsky.social. Visit my website: benryan.net
". Dr. Edwards-Leeper advocated for more careful, cautious, and drawn out psychological assessments of children before deciding whether they were good candidates for puberty blockers and cross-sex hormones. "
However, Dr. Edwards-Leeper and all those profiled in the NYT podcast advocating for them (De Vries, Cohen-Kettenis, Leibowitz) cannot tell you what these assessments imply regardlng likely outcomes. Do kids they assess as appropriate for intervention do well? They don't know. Do they do better than they would have without losing function in their previously healthy bodies? They don't know. They just know some patients were helped. They believe.
This is not medicine. Framing the controversy as between those following WPATH (with several key people who wrote the adolescent recommendations being the ones saying to follow it, and others helping to write the Endocrine Society recommendations) and those being more reckless does not describe gender medicine at all. It describes a bunch of true believers who either won't keep track of or won't report (de Vries et al on hormones...where is that study, how about the long term studies of the Dutch kids, which didn't look great?), outcomes.
But let's let them do what they always did because they think it works.
They haven't shown it....too new...but you should trust them...they've been doing it forever.
Which is it?
Cass spelled it out--the assessments can't tell you anything about likely outcomes...Olson-Kennedy said, ok, don't do them...but that's the wrong answer, too.
There are literally tens of thousands of young people in the Us who were put on these interventions as minors. How are they doing now?? The young people with this distress deserve these answers, not confidence in anecdotes from true believer MD's.
They're going to destroy all of the records they can, during this time. The lawsuits are coming.
I'm so relieved that this clinic is shutting down, especially because or is the beginning of exposing what a fraud this woman is and how much damage she has caused.
She will blame everything on Trump and those evil bigots, but really she's covering for being exposed.