

The Association of Health Care Journalists Has Published a Highly Misleading Primer on Covering Transgender Medicine
The Association of Health Care Journalists Has Published a Highly Misleading Primer on Covering Transgender Medicine
One would hope that this leader in promoting fine health and science journalism would do better.


As veteran journalist and Blocked and Reported podcast host Jesse Singal pointed out in detail on Friday on X, a new primer—“Here’s what the limited research we have on transgender health tells us”—on reporting about transgender health care published by the Association of Health Care Journalists on Sept. 12 is a highly misleading and at times outright false document. I will second Singal to say it is a shame, to say the least, that the AHCJ is not promoting circumspect and scientifically precise reporting on this crucial issue.
Below, I will go through the AHCJ reporting primer and point out some of its flaws to supplement what Jesse has already addressed on X.
Some back story: At the AHCJ conference here in New York City in June, I went to one session on the U.S. Transgender Survey study. During the Q&A, I found myself compelled to get to the mic and tell the room how shocked I was that we were at a science journalism conference and at times we were essentially being told to abandon scientific critical thinking on the issue of pediatric gender medicine.
I told the crowded room, for example, that they should examine for themselves what the Society for Evidence Based Gender Medicine truly stands for—this after SEGM was portrayed during the conference session as a bastion of hate and pseudoscience not to be trusted. I relayed how I had gone to SEGM’s conference last fall and found that it amounted to a geeky crash course in evidence-based medicine practices and was not at all ideological or political.
Here is my reporting from the SEGM conference:

While I was at the mic at this AHCJ conference session in June, one of the authors of the new primer on trans reporting howled out objections to my words from the audience. She insisted that gender-transition treatment for kids is life saving—this despite the fact that no study has shown that it is live saving and the one study to assess whether it is (which was first presented at SEGM and which I covered in February when it was published) didn’t find it was. The very next day, this journalist gave a presentation on how to scrutinize flawed and misleading science. She betrayed no sense of cognitive dissonance over this glaring contradiction.
As for the transgender reporting primer she coauthored for AHCJ, below are some notes following screen shotted segments from the primer.
1. Promoting the at-times incoherent Science editorial
This editorial in Science, written by a pair of leaders in the gender-medicine field, is laden with misleading claims and a general incoherence in its arguments. I would hope that science and medical journalists would be able to detect these problems.
For example, the Science essay claims that there is “mischaracterization of [trans and gender-diverse] health science by non-expert, anti-TGD political activists as lacking supportive evidence and potentially causing harm.”
And yet in its opening paragraph, the AHCJ primer refers to Britain's Cass Review. This 388-page document, which concluded that pediatric gender-transition treatment is based upon “remarkably weak evidence,” was written by the UK’s leading pediatrician following a four-year effort. It was based on seven systematic literature reviews written by evidence-based medicine, or EBM, experts at the University of York. Those reviews joined with five other such previous reviews, also written by EBM experts, in finding that the science behind pediatric gender medicine is weak and inconclusive.
So it is highly misleading to suggest that only “nonexperts” have come to such a conclusion.
The Cass review has been the target of a fierce misinformation campaign, as I’ve demonstrated:


It’s important to remind health care journalists that the burden is on those who support wide access to puberty blockers and cross-sex hormones for gender dysphoric children to demonstrate that such powerful interventions are supported by evidence strong enough that families and doctors can make fully informed decisions about whether the apparent benefits of pediatric gender-transition treatment outweigh the risks, such as infertility or sexual dysfunction and the possibility of regretful detransitioning one day.
2. Omitting who the gender-transition bans target
This passage omits the crucial detail that the vast majority of state bans on gender-transition treatment concern minors, not adults. Since 2021, Republicans in 24 states have passed bans on minors accessing puberty blockers, cross-sex hormones and gender-transition surgeries to treat gender dysphoria. Two others, Arizona and New Hampshire, have only banned such surgeries for minors.
It is the more uncommon state, such as Florida, that has passed a law that at the very least complicates adult access to cross-sex hormones. That state’s law, for example, requires that only MDs write such prescriptions; whereas most trans adults get their hormones from nurse practitioners and there aren’t enough MDs to meet the demand.

3. Falsely claiming Europe’s policies are the sole byproduct of politics

Four Scandinavian nations and the United Kingdom have recently engaged in an about-face and begun sharply restricting access to gender-transition treatment for minors (again, the AHCJ primer doesn’t mention that these policies are specific to kids). But for the most part, these policies were not put in place by politicians, but by the nations’ health authorities—in response to the systematic literature reviews that demonstrated that pediatric gender medicine is based on a shaky evidentiary foundation.
The exception is that after England’s National Health Service began officially forbidding its physicians from prescribing puberty blockers to gender dysphoric minors in the spring, the outgoing Tory government passed an “emergency” ban on private clinics prescribing such drugs. The new Labour government has extended the ban through November. But the vast majority of Britons get their healthcare from the NHS. So this ban only impacts this issue around the margins.
The NHS is planning a clinical trial of puberty blockers that, should it pass muster with an ethical review board, is meant to launch in 2025. Time will tell if the oft-delayed NHS will meet that schedule.
4. Credulously citing Tordoff, and doing so incorrectly
Jesse Singal, with a world weariness that is well-earned after having previously explained in such exacting detail why the Tordoff et al paper is deeply misleading and flawed, pointed out on X on Friday how the AHCJ primer is credulously referencing the flawed paper twice while also referencing a World Professional Association for Transgender Health (WPATH)-commissioned systematic literature review, Baker et al, that revealed the weakness of the data behind gender-transition treatment:
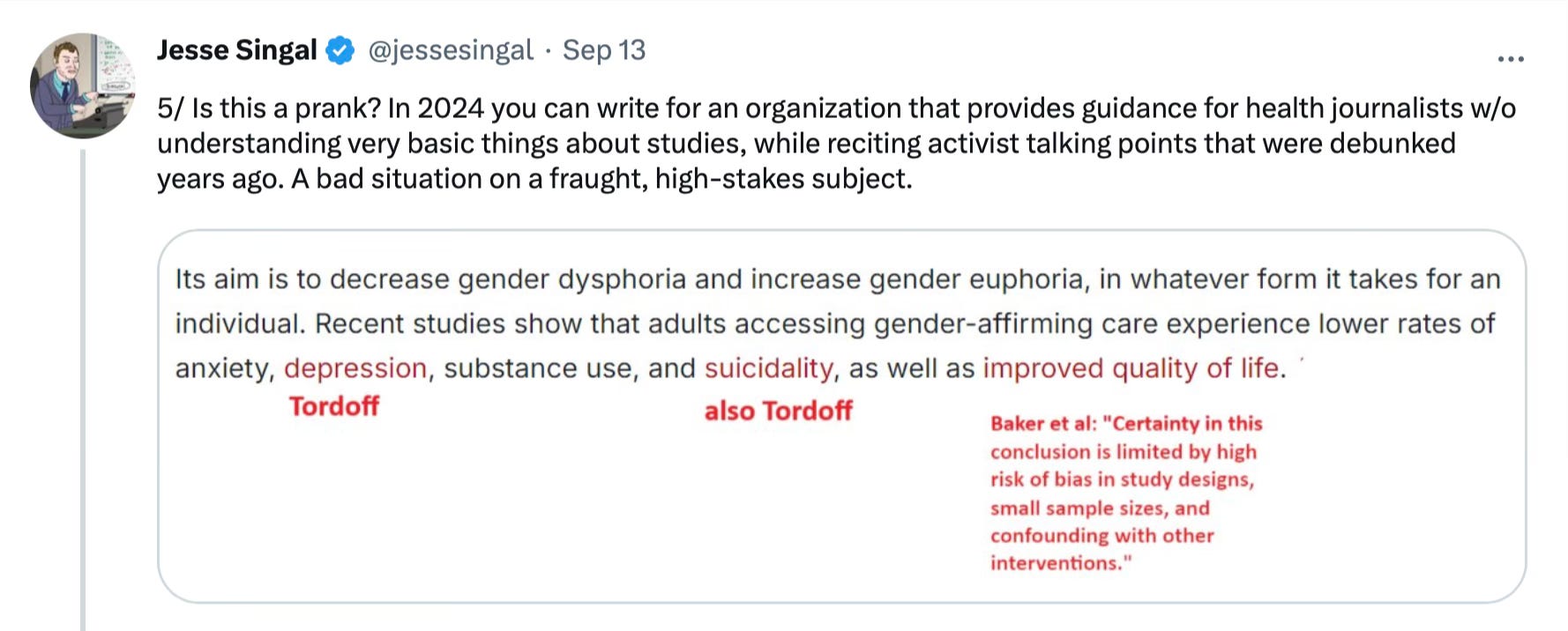
The Tordoff study, first off, did not concern adults, as ACHJ suggests. It was a study of 104 adolescents and young adults 13 to 20 years old, that started with some of them having received gender-transition treatment. After 12 months, 69 had started such medications.
The study authors claimed that in comparison to the untreated group, the treated youths had lower suicidality and depression. But as Singal has reported, the mental-health markers of the treatment group did not change over the 12 months. What changed was the composition of the untreated comparison group, which was plagued by considerable loss to follow-up. At the 12-month mark, just five participants in the untreated comparison group provided mental-health-related data; and this small group was especially unwell in that regard. It remains possible that those who left the study did so because they were feeling well, thus biasing the study findings.
5. Not mentioning sexual function and fertility as major risks
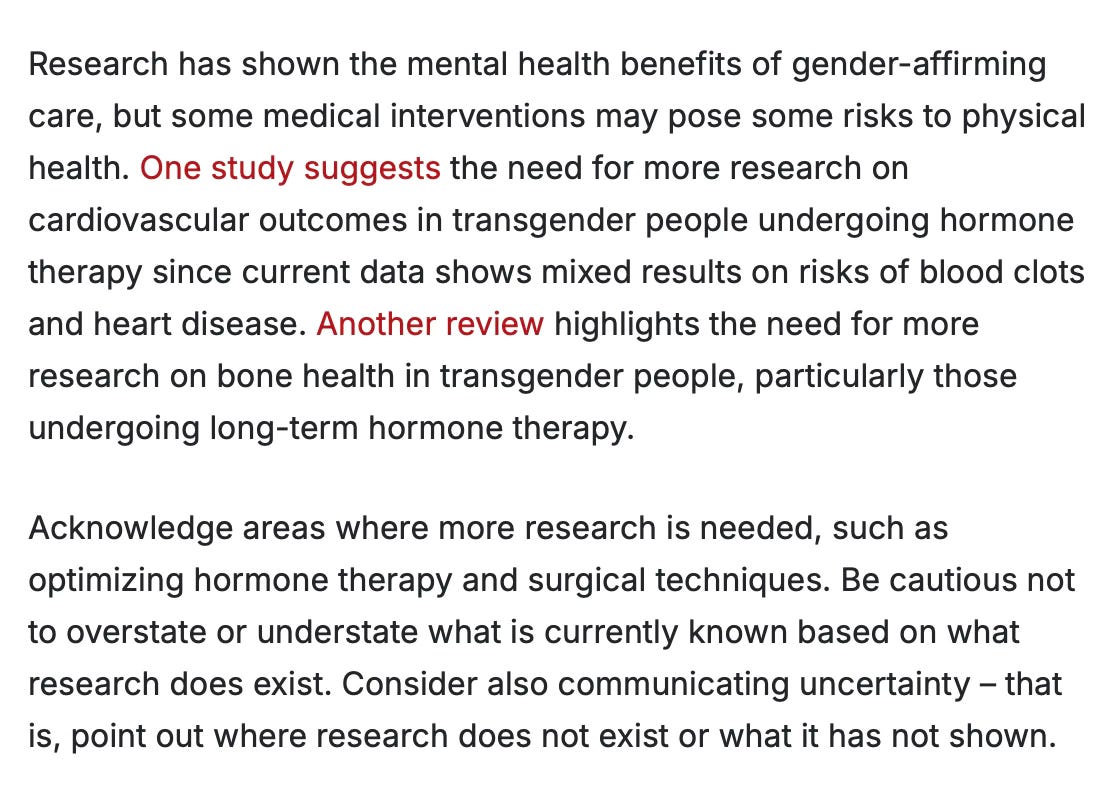
The most central ethical concern about whether to prescribe puberty blockers and cross-sex hormones to minors in particular is that doing so, especially when starting blockers at the immediate onset of puberty among natal males, poses a risk of causing infertility. Major leaders in pediatric gender medicine, such as UCSF’s Dr. Jack Turban, who often glosses over the potential downsides of gender-transition treatment for children, acknowledge this risk. Sexual dysfunction is also a major risk of such pediatric treatment. And yet the AHCJ primer mentions neither of these risks.

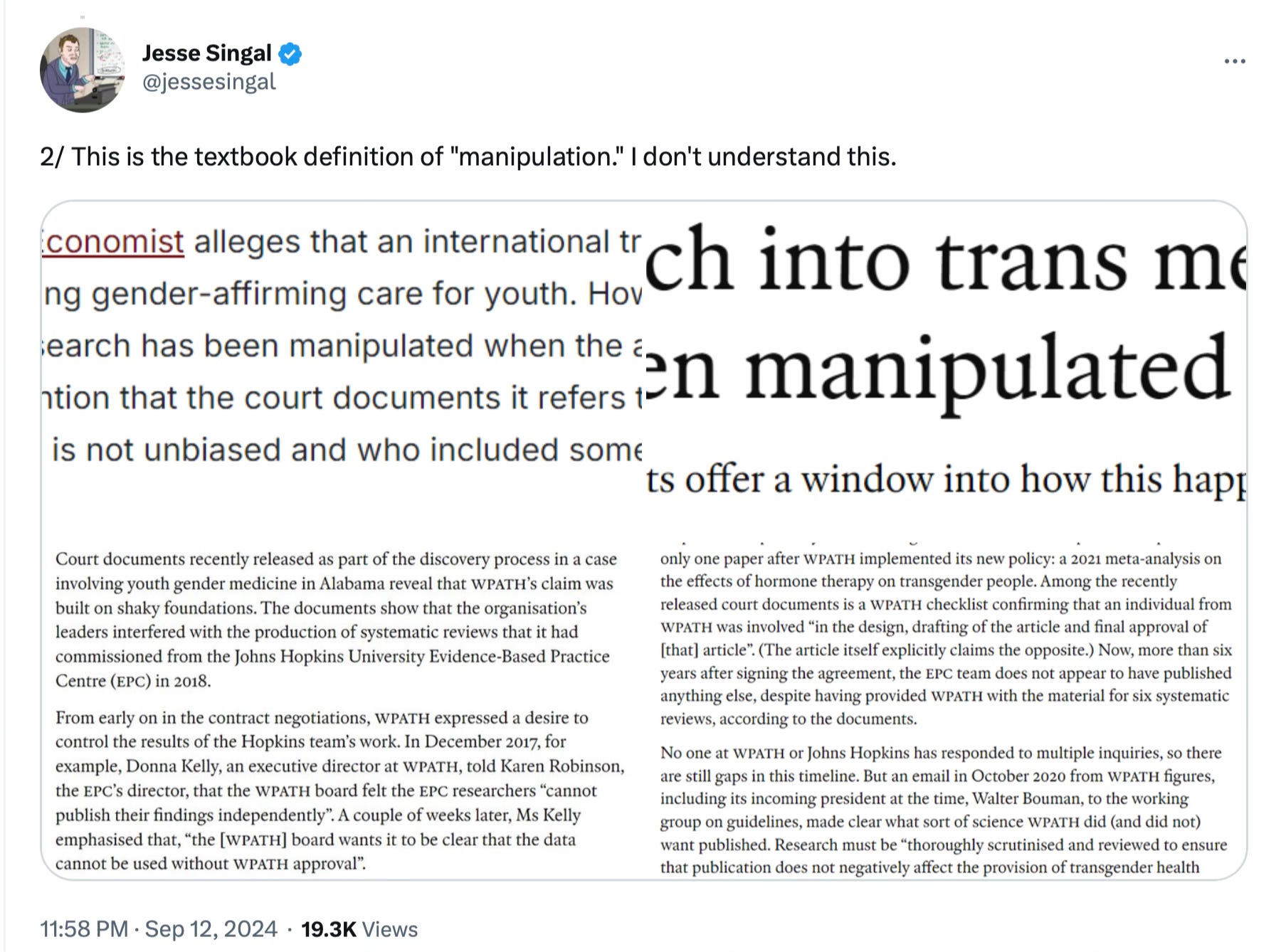
6. Falsely claiming Singal’s Economist article was incorrect

In June, Singal reported in The Economist about how internal WPATH emails subpoenaed by the Alabama Attorney general and unsealed that month showed that the organization manipulated the systematic literature reviews that it had commissioned about gender medicine from EBM researchers at Johns Hopkins. The Hopkins team was conducting research—it was research about research—and WPATH did manipulate that research. AHCJ is incorrect to claim otherwise.
Singal was not amused by AHCJ publishing false claims about his reporting:
Also, regardless of who retrieved the WPATH emails and how they packaged them in a legal brief, those emails can stand on their own and provide fertile fodder for exacting reporting such as Singal’s about what has gone on behind closed doors at WPATH.
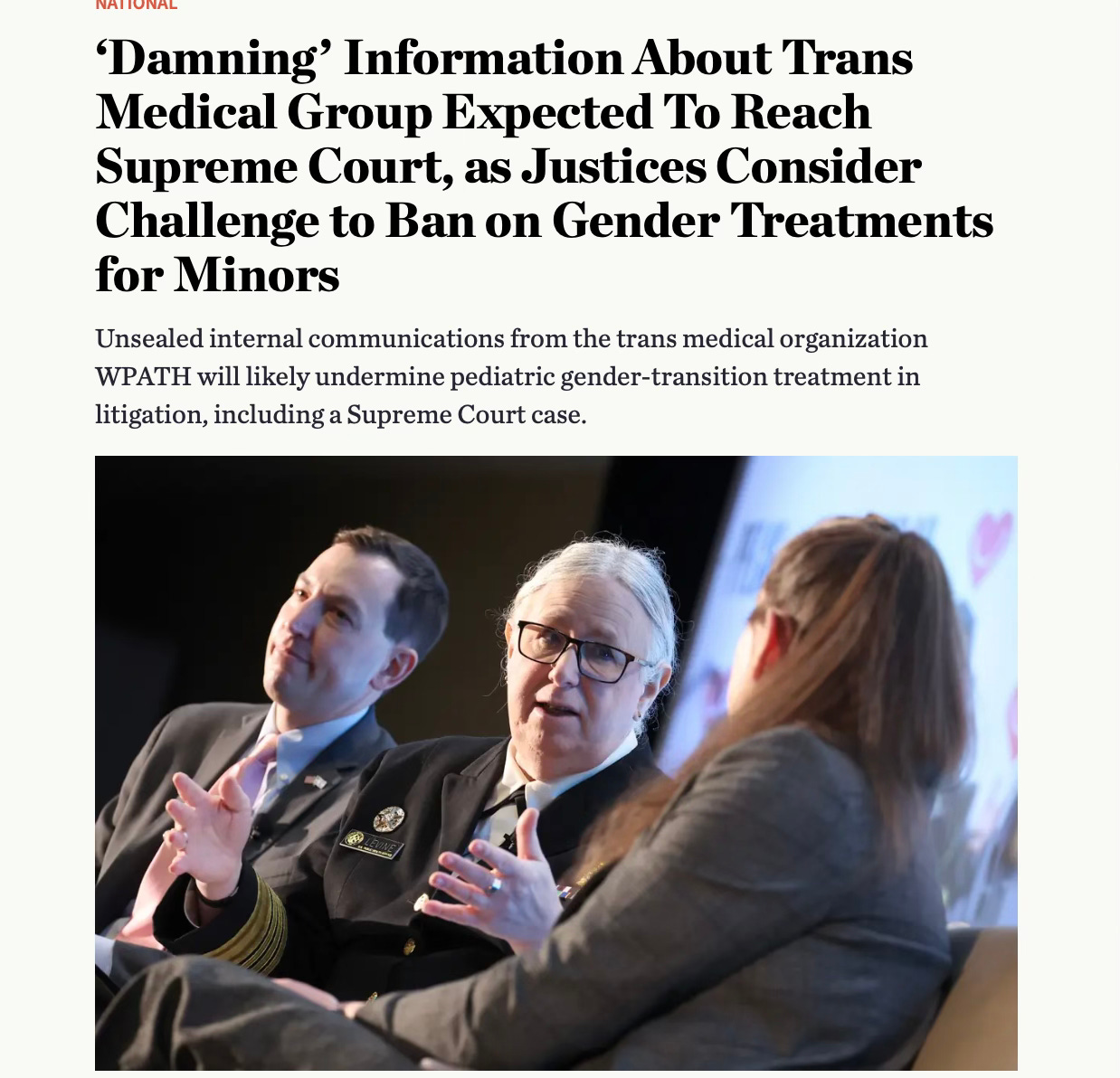
I also reported on those subpoenaed internal WPATH documents:
7. Falsely claiming gender-affirming surgery is rare
As I reported recently, Harvard misled the public to believe that gender-transition surgery in minors is both rare and dramatically less common than natal boys getting gynecomastia surgery:
How Harvard Teed Up the False Claim That the 'Vast Majority of Minors Getting Gender-Affirming Surgeries Are Cis Kids'

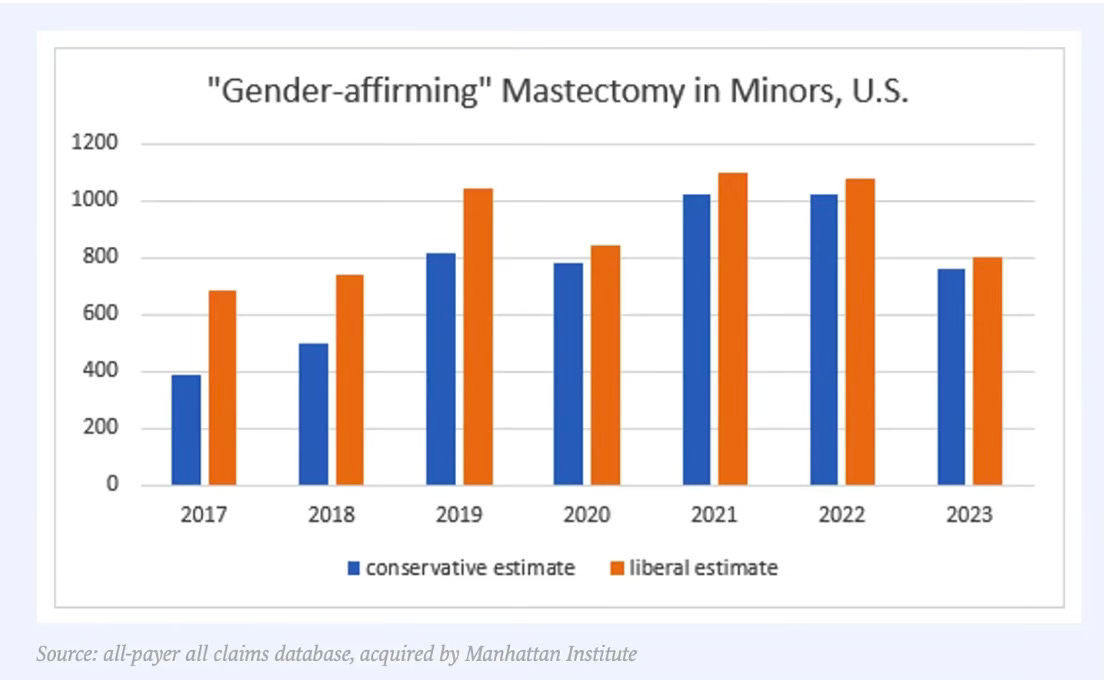
As the Manhattan Institute’s Leor Sapir has found in his analysis of national insurance claims data, double mastectomies, aka top surgery, for natal girls with gender dysphoria are increasingly common:
“A new analysis by the Manhattan Institute, using a more up-to-date all-payer national insurance database from 2017 to 2023, found evidence of 5,288 to 6,294 “gender-affirming” double mastectomies for girls under age 18. This includes 50 to 179 girls who were 12.5 or younger at the time of their procedure.”
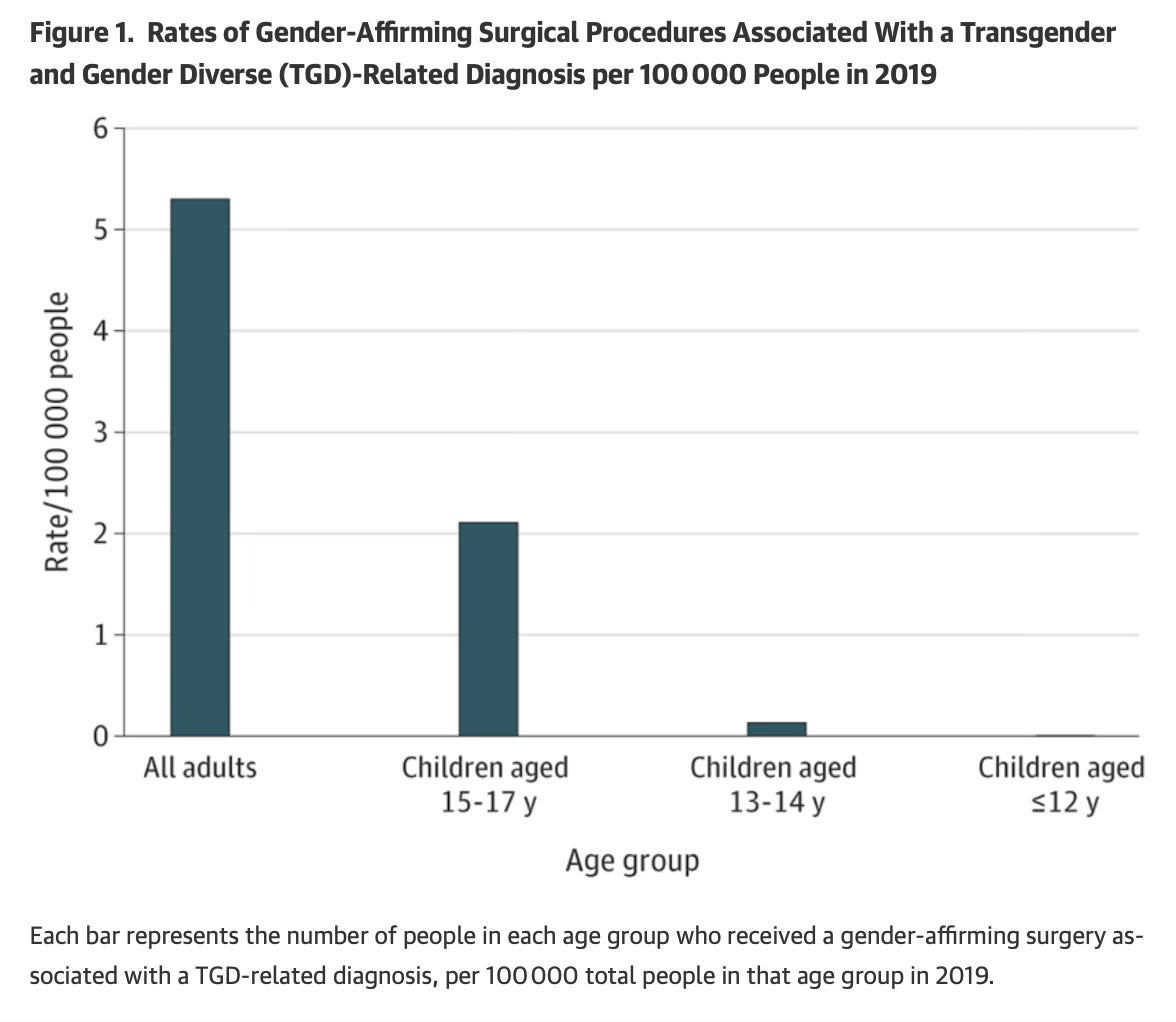
A recent Harvard analysis found that, in 2019, per capita gender-transition surgeries in minors in their mid-to-late teens weren’t even that much less common than those conducted in adults:
8. Reporting uncritically on criticisms of Cass
The AHCJ cites a flawed Mother Jones article written by a cub reporter who cites Dr. Turban as a major source of criticism of the Cass Review, not noting the UCSF child psychiatrist’s glaring conflict of interest: His own work was deemed to be of low quality by the literature reviews that fed into the Cass Review. Dr. Turban has failed to make note of this conflict in numerous forums in which he has sought to undermine Cass, including a debate on gender medicine at MIT earlier this year and the Yale Integrity Project’s efforts to discredit the Review through a non-peer-reviewed white paper they rushed online over the summer.
The MJ article also cites as voices critiquing Cass: the white paper; and its lead author, Yale pediatrician Dr. Meredith McNamara. Jesse Singal has torn the white paper’s criticism of Cass to shreds, and has revealed how Dr. McNamara has been misleading the public in sworn statements regarding what she has strongly suggested is her extensive experience as a pediatric gender medicine doctor. But it turns out she has a notable lack of direct experience working with gender dysphoric youth seeking puberty blockers; she has only ever referred two such patients to a gender clinic during her entire career, per her sworn deposition in the suit over Alabama’s ban of pediatric gender-transition treatment (which was unsealed along with the internal WPATH docs over the summer).
Another of MJ’s sources is Boston University’s Dr. Carl Streed, who as the current president of the U.S. branch of WPATH, USPATH, also has a glaring conflict of interest that goes unacknowledged in the MJ article, given how much the Cass Review excoriated WPATH for its poor observation of scientific principles.
The AHCJ primer also fails to note that no more than a couple dozen members of the British Medical Association, which is a trade union and not a science organization, voted to scrutinize the Cass Review. The BMA’s move has led to an internal revolt, resignations in protest, and a letter objecting to the Cass scrutiny signed by over 1,000 members.

It is also woefully false for AHCJ to claim that the Cass Review, which was published April 9, 2024, could have possibly “fueled much of the legislation” against gender-transition treatment in the United States. Almost all of the current 26 state bans were passed before the Cass Review was published.
Update, Sept. 17: The AHCJ made extensive edits to the reporting primer. But there are still many problems in the document:

To contact AHCJ to express your concerns:
If you would like to express your concerns over the AHCJ primer on reporting on trans medicine, you can email the organization, perhaps by sending them this article, or by posting this article on X (note that the link won’t generate a thumbnail preview, so please screenshot the article and add that image to the link in the tweet) and tagging them. You can also retweet my tweet thread about this Substack: https://x.com/benryanwriter/status/1835021132132671816
Managing editor Erica Tricarico: erica@healthjournalism.org
Digital editor Kevin Ridder: kevin@healthjournalism.org
Director of education and content Katherine Reed: katherine@healthjournalism.org
Executive director Kelsey Ryan (no relation): kelsey@healthjournalism.org; X: @kelsey_ryan
AHCJ general email: info@healthjournalism.org
X: @AHCJ
I am an independent journalist, specializing in science and health care coverage. I contribute to The New York Times, The Guardian, NBC News and The New York Sun. I have also written for the Washington Post, The Atlantic and The Nation.
Follow me on Twitter: @benryanwriter.
Visit my website: benryan.net
Thank You for your thorough reporting on this!
Thank you for the work you do. It appears that journalists like yourself, Jesse Singal, and Bernard Lane in Australia, who actually understand the tenets of evidence based medicine, are a tiny minority. Where I live in New Zealand, the Cass report might as well never have happened for all the attention it has received in the mainstream press.