


Detransitioner Sues Johanna Olson-Kennedy, a Top Pediatric Gender Medicine Doctor, For Medical Negligence
Dr. Olson-Kennedy is the most prominent doctor yet to be sued by a detransitioner—for medical negligence after overseeing a mentally ill girl's gender-transition starting at 12 and mastectomy at 14.

Dr. Johanna Olson-Kennedy, who is one of the most prominent and influential physician-researchers in pediatric gender medicine, has been hit with a damning lawsuit by a former patient. The plaintiff reports having suffered from severe, worsening mental illness while Dr. Olson-Kennedy oversaw her gender-transition treatment, including a double mastectomy at age 14. Now a college student, she recently detransitioned.
The lawsuit accuses Dr. Olson-Kennedy of prescribing the plaintiff, then a newly-gender-questioning 12 year old, puberty blockers following a single cursory appointment and no assessment with a mental health professional; of coercing the girl’s wary parents into consenting to testosterone therapy by insisting their child, who had no history of suicidality, would kill herself without such irreversible treatment; and of failing to provide the family with proper informed consent.
It was only after the girl started taking testosterone at age 13 and had her breasts surgically removed the following year that she actually became suicidal and tried to take her own life, according to the suit. The girl reportedly suffered increasingly severe psychosis, including auditory and visual hallucinations. Dr. Olson-Kennedy ultimately recommended a hysterectomy when the girl was 17.
An outspoken advocate for minors’ access to gender-transition treatment and surgery, Dr. Olson-Kennedy has a history of downplaying potential or certain fertility loss resulting from gender-transition interventions on minors and of minimizing the impact of any regret following so-called top surgery. And she is on record exaggerating the risk of suicide death among adolescents with gender dysphoria and making definitive claims—absent definitive supporting research—that these gender treatments and surgeries save children’s lives. (Specific details and references about these claims of hers are in the final sections of this article.)
Given Dr. Olson-Kennedy’s extensive record of such bold claims and her prominence in pediatric gender medicine, the lawsuit against her—out of the two-dozen similar lawsuits filed thus far by young detransitioners—has the potential to cause some of the greatest damage to the overall reputation and credibility of this controversial and increasingly besieged medical field.
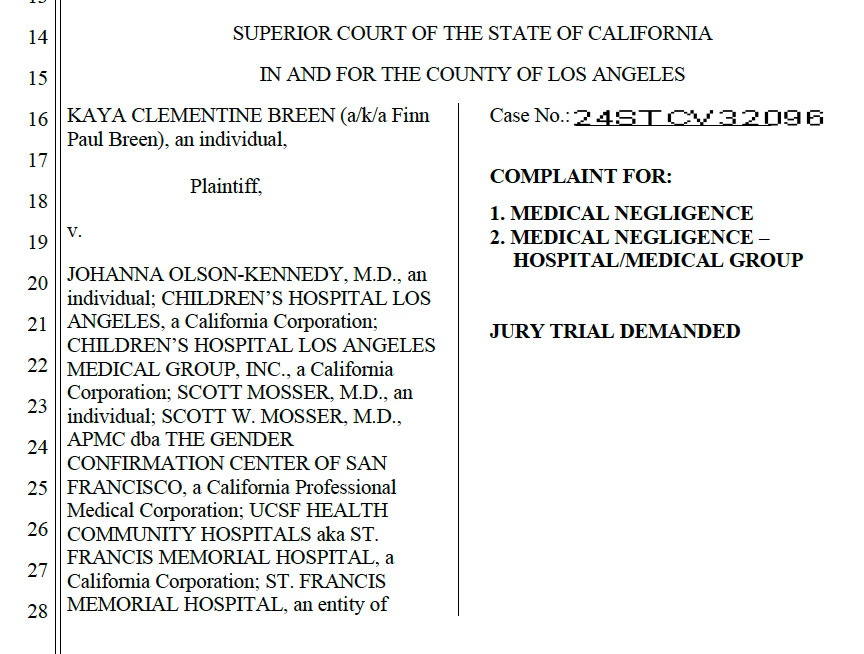
Kaya Breen, 20, who goes by her middle name, Clementine, filed suit on Thursday in Superior Court of the State of California in Los Angeles against Dr. Olson-Kennedy and two of her colleagues, including a surgeon and psychotherapist.
Ms. Breen, who was sexually abused around age 6 or 7, a history that her lawsuit asserts “was never explored, addressed, or discussed” by the defendants, has accused the team of medical negligence. Her suit, which was first reported by Jesse Singal in The Economist on Friday, seeks damages and a jury trial.
Amid declining mental health, Ms. Breen received gender-transition-treatment from Dr. Olson-Kennedy throughout her adolescence—and at times, was under the care of the two other defendants as well. Having identified as male during this period, Ms. Breen ultimately reverted to identifying and presenting as female by the end of her teens. She reports profoundly regretting the treatment—known as gender-affirming care—that she received.
Dr. Olson-Kennedy is the medical director at The Center for Transyouth Health and Development at Children’s Hospital Los Angeles, the nation’s largest pediatric gender clinic, and a professor of clinical pediatrics at the University of Southern California Keck School of Medicine. She is an executive board member of the World Professional Association for Transgender-Health (WPATH) and president-elect of its U.S. branch, USPATH. WPATH is a controversial quasi-activist-medical organization that is largely based in the United States and publishes widely referenced trans-care guidelines. She has reported prescribing cross-sex hormones to over 1,000 adolescents and young adults since 2006.
Dr. Olson-Kennedy is married to a transgender man, Aydin Olson-Kennedy, who is a licensed clinical social worker, a WPATH member and also works in pediatric gender medicine.
Here is a 2020 interview with the Olson-Kennedys:


The lawsuit
Ms. Breen’s suit against Dr. Olson-Kennedy also names as defendants Dr. Scott Mosser, a plastic surgeon at the Gender Confirmation Center of San Francisco, who performed Ms. Breen’s mastectomy; and Susan P. Landon, a licensed marriage and family therapist, who came recommended by Dr. Olson-Kennedy and provided Ms. Breen ongoing counseling. Both Dr. Mosser and Ms. Landon are WPATH members. Ms. Landon was one of Mr. Olson-Kennedy’s mentors in his psychotherapy training.
Additionally, the suit names the various organizations where these professionals worked while caring for Ms. Breen. On top of the aforementioned affiliations, this includes St. Francis Memorial Hospital and UCSF Health Community Hospitals. And there are various John Does who may later be named.
As with all known detransitioner lawsuits against other health and mental health providers, Ms. Breen’s lawsuit alleges that Dr. Olson-Kennedy and her colleagues’ treatment of Ms. Breen did not meet the standards of care in their respective disciplines. This includes accusations that Dr. Olson-Kennedy did not obtain proper informed consent or properly educate Ms. Breen and her parents about the risks of the recommended medical interventions.
Accusing Dr. Olson-Kennedy and her colleagues of “grossly negligent and fraudulent, malicious, and oppressive acts,” the suit characterizes the overall care that the team provided Ms. Breen as heedless, coercive and destructive to her well-being and her body.
Attorneys at Campbell Miller Payne, a Texas firm established by a quartet of former white-shoe lawyers for the sole purpose of representing detransitioners, are representing Ms. Breen. Among their other clients are Isabelle Ayala, who has sued the American Academy of Pediatrics and Brown University pediatrician Dr. Jason Rafferty, who is the sole author of the AAP’s 2018 policy statement on the gender-affirming care method; and Prisha Mosley, whose case in North Carolina was the first detransitioner suit in the nation to be approved to go to trial.

Many of the detransitioner lawsuits filed to date concern natal girls who have suffered from severe childhood trauma, including sexual abuse or assault, and who suffer from a complex web of severe psychiatric conditions and sometimes autism as well.
Clementine’s story
Ms. Breen’s suit alleges:
Clementine’s providers deliberately, grossly, and recklessly breached the standard of care in this case as discussed above, by among other things, failing to adequately assess and treat Clementine’s complex array of mental health symptoms and prior trauma before prescribing irreversible and life-altering medications and performing surgery.
Ms. Breen, whom the lawsuit reports experienced no significant gender incongruence prior to puberty, first began having questions about her gender when she was 11, around the same time she came out as gay. As she moved into puberty, she increasingly suffered from depression, anxiety and other major psychological problems.
Apparently struggling in particular with the sexual abuse she had suffered in early childhood and attendant fears of becoming a woman, she told a school counselor she thought life would be easier as a boy. The counselor told her she was transgender. Her parents, surprised by this news, ultimately took her to see Dr. Olson-Kennedy at her gender clinic just after their child turned 12.
A few minutes into the first 30-minute appointment, which Ms. Breen attended without her parents in the room, Dr. Olson-Kennedy diagnosed her with gender dysphoria and recommended a surgically implanted puberty blocker.
The suit states of the care Dr. Olson-Kennedy provided:
She did not ask about things like past trauma, abuse, or mental health struggles or diagnoses. She involved no other providers or health care professionals in this purported gender dysphoria diagnosis and recommendation for puberty blockers. Instead, she simply took a handful of platitudinal statements from a scared, confused, and traumatized barely-12-year-old girl to give a life-altering diagnosis and handed her the prescription pad. In short, it took Dr. Olson-Kennedy and the team at LA Children’s a single visit to send Clementine down a life-altering, traumatic, body-disfiguring, and irreversibly damaging path of transgender medicalization.
Dr. Olson-Kennedy ordered Ms. Breen’s puberty blocker that very day. It went into the girl’s arm at her next appointment, a little over two months later, and remained there for more than four years. (According to the Mayo Clinic, these implants should typically be replaced annually.) Puberty blockers are known to lower bone density. But while Dr. Olson-Kennedy did order a bone-density scan to take a baseline level, there are no records that she ever ordered any follow-up scans.
At Ms. Breen’s third appointment, six months after the child was put on the puberty blocker, Dr. Olson-Kennedy urged her to start testosterone. In the face of Ms. Breen’s reported reluctance, she said that beginning earlier would help her fully pass as male. To convince her reluctant parents, Dr. Olson-Kennedy told them, in the words of the lawsuit, “that if they did not agree to cross-sex hormone therapy, Clementine would commit suicide.” They relented and their child started the treatment shortly after turning 13.
Just before Ms. Breen turned 14, Dr. Olson-Kennedy recommended a double mastectomy, again emphasizing the importance and benefits of doing this early—to help her obtain a “natural…cis male-looking chest.” Ms. Landon and Dr. Olson-Kennedy wrote referral letters for surgery with Dr. Mosser, who, the suit asserts, never met with Ms. Breen until an approximately 30-minute exchange the day of the operation.
Jesse Singal reports in The Economist:
Perhaps the lawsuit’s most damning claim is that Dr Olson-Kennedy misrepresented Ms Breen’s gender-identity history in the letter of support she wrote to Ms Breen’s surgeon. In the letter, quoted in the complaint and also obtained in full by The Economist, Dr Olson-Kennedy writes that Ms Breen had “endorsed a male gender identity since childhood”—language intended to signal that a young person’s gender identity has been stable for a long time, alleviating concerns that the patient might change their mind after undergoing a permanent procedure. But the claim was contradicted by Dr Olson-Kennedy’s own records
None of these interventions, the suit states, helped Ms. Breen’s mental health. On the contrary.
According to the suit:
For the first time in her life, Clementine began feeling symptoms of depression, intense anger, and thoughts of suicide. She could not focus. For the first time, she began self-harming. After her double mastectomy, she began suffering from symptoms of psychosis. During this time, she grew to hate her body more and more, leading to severe body image issues, which led to obsessively working out and adopting an abnormally low-calorie diet. When she brought up these feelings and struggles with Ms. Landon or Dr. Olson-Kennedy, they were simply dismissed as Clementine’s being jealous of “cis men” or not feeling like she fit in because she was trans.
As Ms. Breen’s mental health spiraled, Dr. Olson-Kennedy’s notes about her check-ups did not betray any substantial alarm, according to the lawsuit.
Finally, Dr. Olson-Kennedy urged Ms. Breen to undergo a hysterectomy when she was 17 years old.
According to the suit:
That prompted Clementine to realize that she likely would want children one day. Dr. Olson-Kennedy, nonetheless, insisted she get a hysterectomy, telling Clementine that having children was probably not possible, due to her having been on histrelin and testosterone for five combined years (something she had not told Clementine years earlier).
By this point, the trust Ms. Breen’s parents held in Dr. Olson-Kennedy had begun to sour. Their child never had her uterus removed.

In late high school, having seen various psychiatrists, Ms. Breen began seeing new outside counselor—a dialectical behavioral therapist—and came to realize that she was not transgender and that, her suit asserted, her apparent gender dysphoria had been driven by the sexual abuse she had suffered.
Ms. Breen tapered her testosterone use. She stopped taking the hormone altogether early this year, at age 19, and fully detransitioned. Her mental health has improved dramatically, according to her lawsuit.
But at 20, Ms. Breen faces living with the now-unwanted physical changes brought on by having only gone through a male puberty and spending years on testosterone. This includes a masculine frame, a deepened voice and an Adam’s apple.
Where were these care providers coming from?
I reached out to Children’s Hospital Los Angeles (CHLA) and Dr. Olson-Kennedy over email, seeking comment. A spokesperson for the hospital replied with a statement.
The Transyouth center where Dr. Olson-Kennedy is the director, the statement said, “has provided high quality, age-appropriate, medically necessary care for more than 30 years. Treatment is patient- and family-centered, following guidelines from professional organizations such as the American Academy of Pediatrics, American Medical Association, and Endocrine Society.”
Otherwise, the organization indicated it could not comment on pending litigation or on private patient matters.
Boston Children’s Hospital (BCH) was the first in the nation to import what’s known as the Dutch model from researchers in the Netherlands and start providing puberty blockers and cross-sex hormones to minors with gender dysphoria. That was in 2007. So the claim that BCH’s Los Angeles counterpart has provided “medically necessary care” for more than three decades cannot be interpreted to mean its physicians have prescribed such medications to minors for even as long as two decades.
Below is a screenshot from a training webinar that Dr. Olson-Kennedy, gave earlier this year, the recording of which was leaked to me. The chart shows the number of referrals to her youth gender clinic per year. As you can see, the clinic only got going with substantial numbers of children about 10 years ago, not 30.

Notably, the CHLA statement made no mention of WPATH’s guidelines, despite their broad influence on U.S. trans-care and Dr. Olson-Kennedy’s leadership within the organization.
Another note on the “medically necessary ” line: WPATH records subpoenaed by Alabama’s attorney general and compiled in an amicus brief recently submitted to the Supreme Court revealed that WPATH’s leadership, in the words of the brief, “made sure to sprinkle the ‘medically necessary’ moniker throughout” the 2022 revision to its guidelines. The purpose was to help secure insurance coverage and win lawsuits. WPATH made the claim about medical necessity despite a paucity of research backing such an assertion.
I also reached out to the Gender Confirmation Center of San Francisco, which sent a link to the following reply:
Dr. Mosser is known for being willing to perform double mastectomies on patients with a BMI as high as 65. Severe obesity raises the risk of complications from many surgeries.
Ms. Landon did not respond to a voicemail seeking comment.
Diagnostic overshadowing
Ms. Breen’s suit against the care team alleges that, their patient’s history of childhood sexual abuse and her myriad psychiatric problems notwithstanding, Dr. Olson-Kennedy in particular apparently engaged in what is known as diagnostic overshadowing. In other words, the physician allegedly focused overwhelmingly on the girl’s gender dysphoria and on treating it with blockers, hormones and surgery. Meanwhile, Dr. Olson-Kennedy reportedly gave the girl’s other mental-health issues the short shrift or apparently presumed that the gender treatments would resolve them.
The suit alleges that Ms. Landon similarly “reduced all of her issues to the notion that all of her problems were perfectly normal for someone who is trans.” Ms. Landon, the suit asserts, did not explore with the child why she might have come to identify as trans or any other reasons why she came to feel uncomfortable in her female body at puberty’s onset.
The care team allegedly refrained from examining whether Ms. Breen’s other mental-health problems might, in fact, have been the source of the gender dysphoria, and not vice versa. Nor did Dr. Olson-Kennedy appear to have considered whether the testosterone might only have worsened those other problems.
“She needed psychotherapy for an extended period of time to evaluate, assess, and treat her complex co-morbid mental health symptoms,” Ms. Breen’s legal complaint says. “Instead, she was fast-tracked” onto the gender-transition treatments.
As a consequence, Ms. Breen’s body “has been irreversibly and profoundly damaged,” the suit asserts. Now a young woman studying acting at UCLA, Ms. Breen wants to have children one day and, according to the suit, is troubled by the fact that if she is even able to conceive and carry a pregnancy, she will not be able to breastfeed. And she suffers from the apparent damaging health impacts of long-term testosterone treatment, including vaginal atrophy, which can make sex painful, and very high cholesterol.
The public has actually already received a preview of Ms. Breen’s story. The influential Canadian anti-gender-transition-treatment activist known as Billboard Chris posted a 6-minute video on X on Oct. 22 (see below) documenting a candid recent exchange between the two of them on the UCLA campus.
“It totally messed my life up,” Ms. Breen told Billboard Chris of the gender-transition treatment she received.
But the lawsuit Ms. Breen was by that time preparing against Dr. Olson-Kennedy and her colleagues only became public on Friday.
Dr. Olson-Kennedy: a prominent and outspoken advocate
Dr. Olson-Kennedy is the leading investigator on a multifaceted, long-running $10 million National Institutes of Health study of the care and treatment of youth who identify as transgender.
As Jesse Singal reported in The Atlantic in 2018, a 2017 paper indicated that the youngest patients receiving cross-sex hormones at Dr. Olson-Kennedy’s clinic during the years prior were 12 years old.
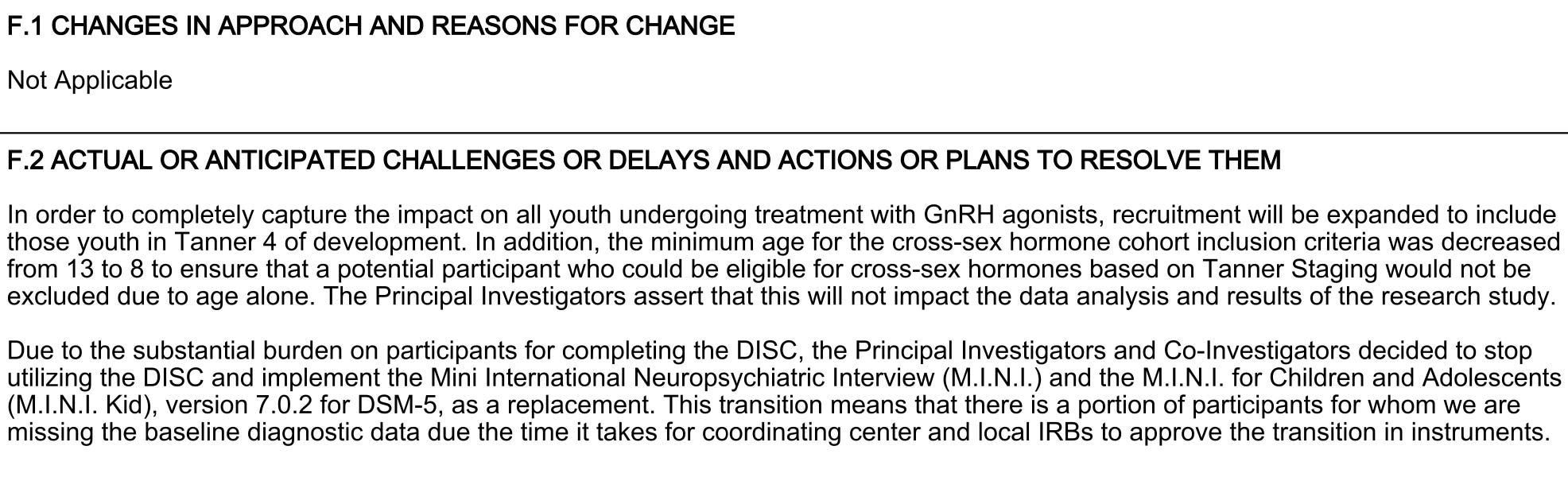
Also in 2017, Dr. Olson-Kennedy sought and received approval for her NIH-funded research to reduce the minimum age for prescribing cross-sex hormones to children from 13 to eight years old.
The New York Times reported on Oct. 24 that Dr. Olson-Kennedy said she had deliberately withheld publishing null findings from a particular NIH-funded study of puberty blockers among minors with gender dysphoria, citing political reasons. However, Dr. Olson-Kennedy asserted in a sworn statement submitted Nov. 17 to a South Carolina civil trial that her words were mischaracterized by the Times and that the long-delayed results had, in fact, not yet been published because, she wrote, of the “sheer amount of work and resources required to do so accurately, transparently and clearly.”
Regardless of the reason why Dr. Olson-Kennedy has not yet published these research findings, hiding—and discouraging—inconvenient research findings is a common pattern in this field, as I reported:

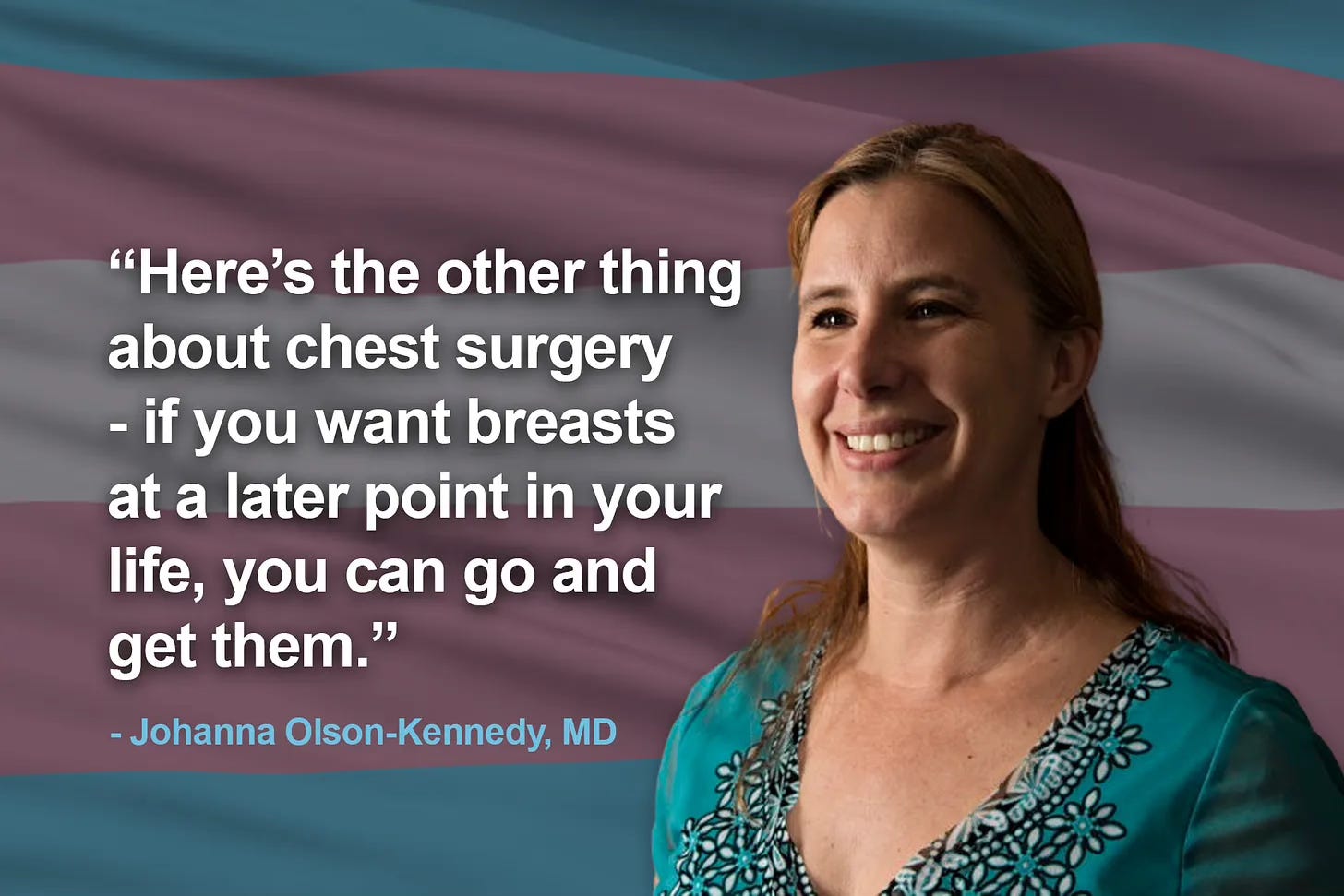
Dr. Olson-Kennedy is perhaps most well known to pediatric gender medicine outsiders because of an undercover video taken in 2018 of a lecture she gave to mental health providers instructing them on how to write letters to help minors obtain insurance coverage for gender-transition interventions. During the lecture, she expressed evident exasperation with prevailing concerns that gender dysphoric minors who have a double mastectomy might later regret the operation.
“What we do know is that adolescents actually have the capacity to make a reasoned, logical decision,” she said. “And here’s the other thing about chest surgery: If you want breasts at a later point in your life, you can go and get them.”
Ms. Breen has tried to go out and get breast reconstruction. But she told Billboard Chris that she has had a much harder time securing the surgery for that than she did when it came to her original mastectomy.
I covered the “go out and get them” video in detail previously:

Natal females who have a double mastectomy as part of a gender transition will likely be unable to breastfeed as a result. According to a 2023 paper out of Australia on post-top-surgery regret: “Most transgender guidelines do not include the impact of chest masculinising mastectomy on breastfeeding as a part of the surgical consent process. Notably, the World Professional Association for Transgender Health (WPATH) Standards of Care makes no recommendation for counselling on breastfeeding before surgery.”
In a video of a 2015 lecture Dr. Olson-Kennedy gave, she further said on the subject:
“Surgery, chest surgery for trans guys as minors, is critical. And it’s available! It’s not nearly as difficult as genital reconstruction, because it doesn’t have anything to do with sterilization. The difficulty of genital surgery is that it is surgical sterilization and people get super worked up about that. And that is the barrier that we have to overcome. And I think we’re going to. But chest surgery is not that.”
“Would you rather have a live son or a dead daughter?”
In a 2011 interview with ABC News, Dr. Olson-Kennedy disclosed to how she speaks with parents of gender dysphoric patients: “We often ask parents, ‘Would you rather have a dead son than a live daughter?’”
As with many other detransitioner lawsuits, such as Chloe Cole’s against Kaiser Permanente and Ms. Ayala’s against Dr. Rafferty and the AAP, the suit against Dr. Olson-Kennedy alleges that the doctor coerced Ms. Breen’s parents by saying to them the flipped version of the notorious, widely uttered mantra: “Would you rather have a live son or a dead daughter?”
In the aforementioned 2015 lecture, Dr. Olson-Kennedy further said of double mastectomies for gender dysphoric minors: “It’s a very easy, safe, relatively fast procedure that is absolutely life saving.”
There is no research that firmly supports the claim that top surgery in this population prevents suicide death among them.
How many minors have gotten top surgery in recent years? My reporting on that question is here:

And here:

Dr. Olson-Kennedy has a long history of insisting that the treatments she provides are life saving and that providing them should be prioritized over preserving fertility. Natal males in particular are at substantial apparent risk of infertility if, as WPATH recommends, they receive puberty blockers soon after puberty’s onset followed by long-term estrogen treatment.
In the 2012 video below, NBC’s Hoda Kotb said to Dr. Olson-Kennedy: “To me it seems ridiculous to have a kid at age 12, 13, 14 deciding whether they want to have biological children when they’re 20, 30 or 40.”
Dr. Olson-Kennedy immediately replied: “Well, they make the decision to kill themselves at 12 and 13. That’s a pretty powerful decision.”
“We take an oath: first do no harm,” Dr. Olson-Kennedy continued. “If doing nothing is doing harm, you have to do something.”
Ms. Breen’s lawsuit alleges that what Dr. Olson-Kennedy should have done in her case was nothing where gender treatments were concerned. Instead, the suit asserts, the doctor should have treated her underlying mental health problems.
“I don’t know how a child can consent to the loss of their fertility,” Ms. Breen told Billboard Chris in October. “Children can’t conceptualize that.”
Dr. Olson-Kennedy further told ABC in 2011 of children with gender dysphoria: “These kids have a suicide rate that is astronomical compared to any other group.”
Two recent studies, one in England and the other in Finland, recently found that the suicide rate among gender-distressed minors is elevated compared with their age-matched peers; and yet suicide deaths among them are nevertheless rare.
In Wednesday’s oral arguments at the U.S. Supreme Court over Tennessee’s ban on pediatric gender-transition treatment, ACLU litigator Chase Strangio, a trans man, said that “completed suicide is thankfully and admittedly rare” among children who identify as transgender.
What’s more, the Finnish study, which I covered for The New York Post and which no one during the Supreme Court’s oral arguments seemed to be aware of, is the only study to date to assess whether there is independent, statistically significant association between receiving gender-transition treatment and a difference in the suicide death rate among young people. The study authors found there was not.


A history of denigrating assessments for gender dysphoric kids
Dr. Olson-Kennedy also has a history of doubting the value of the biopsychosocial assessments that WPATH recommends for minors before they receive gender-transition treatment or surgeries. She shares this in common with UCSF child psychiatrist Jack Turban, who suggested in his recent book that the assessments were worthless and should be done away with.

Jesse Singal reported in The Atlantic in 2018:
Olson-Kennedy is not convinced that mental-health assessments lead to better outcomes. “We don’t actually have data on whether psychological assessments lower regret rates,” she told me. She believes that therapy can be helpful for many TGNC [trans and gender nonconforming] young people, but she opposes mandating mental-health assessments for all kids seeking to transition. As she put it when we talked, “I don’t send someone to a therapist when I’m going to start them on insulin.” Of course, gender dysphoria is listed in the DSM-5; juvenile diabetes is not.
Then there is a 2019 podcast interview that Dr. Olson-Kennedy gave to members of the controversial gender clinic Gender GP, which has provided gender-transition treatment to British minors via telemedicine from abroad. Marianne Oakes, the organization’s lead counselor, said in reference to guardrails around gender-transition treatment: “I feel the system is geared up to protect cis people from making a mistake rather than actually caring for the trans people.”
To which Dr. Olson-Kennedy replied: “A hundred percent, absolutely.” She continued: “I always say what is there in that concern?…What does it mean to make a mistake? What does that mean? So we’re gong to accidentally make someone trans?” She attributed such concern about the potential harms of pediatric gender-transition treatment to what she called “cis fragility.” And she said that these worries are what “drives people to create huge and unmanageable and often inaccessible assessment periods” for minors seeking gender-transition treatment.
Dr. Olson-Kennedy continued: “It never takes into account autonomy of humans—that let’s talk about what it would mean if we just let people move forward and we affirm and believe what they were telling us, right? At the end of the day, who is responsible for that? The person that made that decision.”
In Ms. Breen’s case, her lawsuit against Dr. Olson-Kennedy and her colleagues disagrees. It asserts that those adults were responsible for what became of Ms. Breen’s childhood and seeks to hold them accountable.
I am an independent journalist, specializing in science and health care coverage. I contribute to The New York Times, The Guardian, NBC Newsand The New York Sun. I have also written for the Washington Post, The Atlantic and The Nation. Follow me on Twitter: @benryanwriter and Bluesky: @benryanwriter.bsky.social. Visit my website: benryan.net
The level of professionalism and use of unbiased language in your writing is amazing in this context. After any given sentence I half expect the next to read "Can you believe the nerve of these f*****g lunatics?"
It is so important that you continue writing the way you do, as it is the only way to bring more sane people into the light. The events described are so horrific, any other presentation might lead to undue skepticism by the reader. I'm sure more inflammatory language could get more clicks, but not change more minds. We owe it to kids like Clementine to support your work.
Good. Take this ghoul for everything she’s worth.
The “you can just go get breasts later” comment has haunted me since I first heard it. It’s so emblematic of the way this movement views the body: not as a holistic, functional organism, but as a corkboard onto which one pins and un-pins various signage. Body parts are purely symbolic. Breasts aren’t meant to produce nourishment for, comfort, and help you bond with your babies. They aren’t meant to provide sexual pleasure for you and your partner. They aren’t meant to respond to the hormonal rhythms of your body and in so doing let you know what’s going on with your cycle, with a pregnancy, etc. Breasts are a pair of lumps on the front of a person’s torso that signal to the world that the person identifies as a woman. If the person doesn’t identify as a woman, remove them. If they subsequently identify as a woman again, just affix some new lumps so people will know. It doesn’t matter that they won’t be *actual breasts, that function*; they’re just there to communicate your gender identity. It’s such an impoverished and grotesque way to conceive of the human body.