
Top Plastic Surgeon Won't Commit to Opposing Bans of Gender-Transition Treatment For Minors, Plus He Decries WPATH For Lack of Transparency
American Society of Plastic Surgeons president Steven Williams evoked Tuskegee when asserting that gender doctors can't always be trusted to self-regulate. He said state regulation might be warranted.

The president of the American Society of Plastic Surgeons has declined to assert that the organization’s recent public statements regarding pediatric gender medicine categorically signaled its opposition to bans of gender-transition treatment for minors. The top plastic surgeon also left the door open for supporting a nationwide ban—but not criminalization—of providing such medical interventions to those under age 18, should future research findings indicate that such legislation were warranted.
“Currently, ASPS doesn’t think that gender-affirming care for adolescents is appropriate.” —Dr. Steven Williams, president of the American Society of Plastic Surgeons
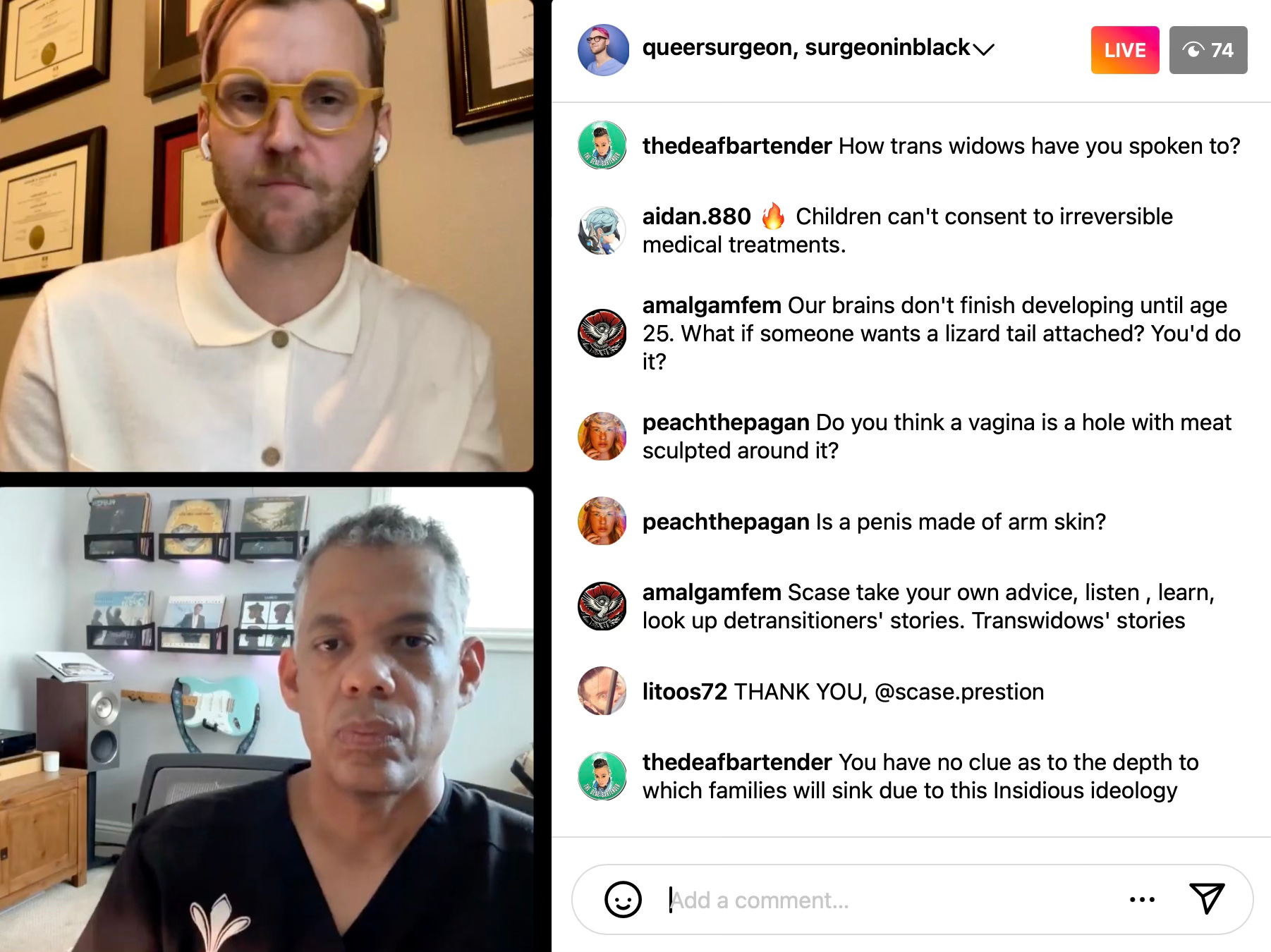
These reflections from Dublin, California, plastic surgeon Dr. Steven Williams came during his frank yet congenial hour-long Instagram Live conversation on Thursday evening with gender-affirming surgeon Dr. Blair Peters. Both doctors called for greater care and respect for transgender people. But Dr. Williams, who is ASPS’s first Black president, evoked the egregious history of mistreatment of African Americans at the hands of the U.S. medical establishment to call into question whether physicians in general—and gender-transition doctors in particular—can always be trusted to self-regulate.

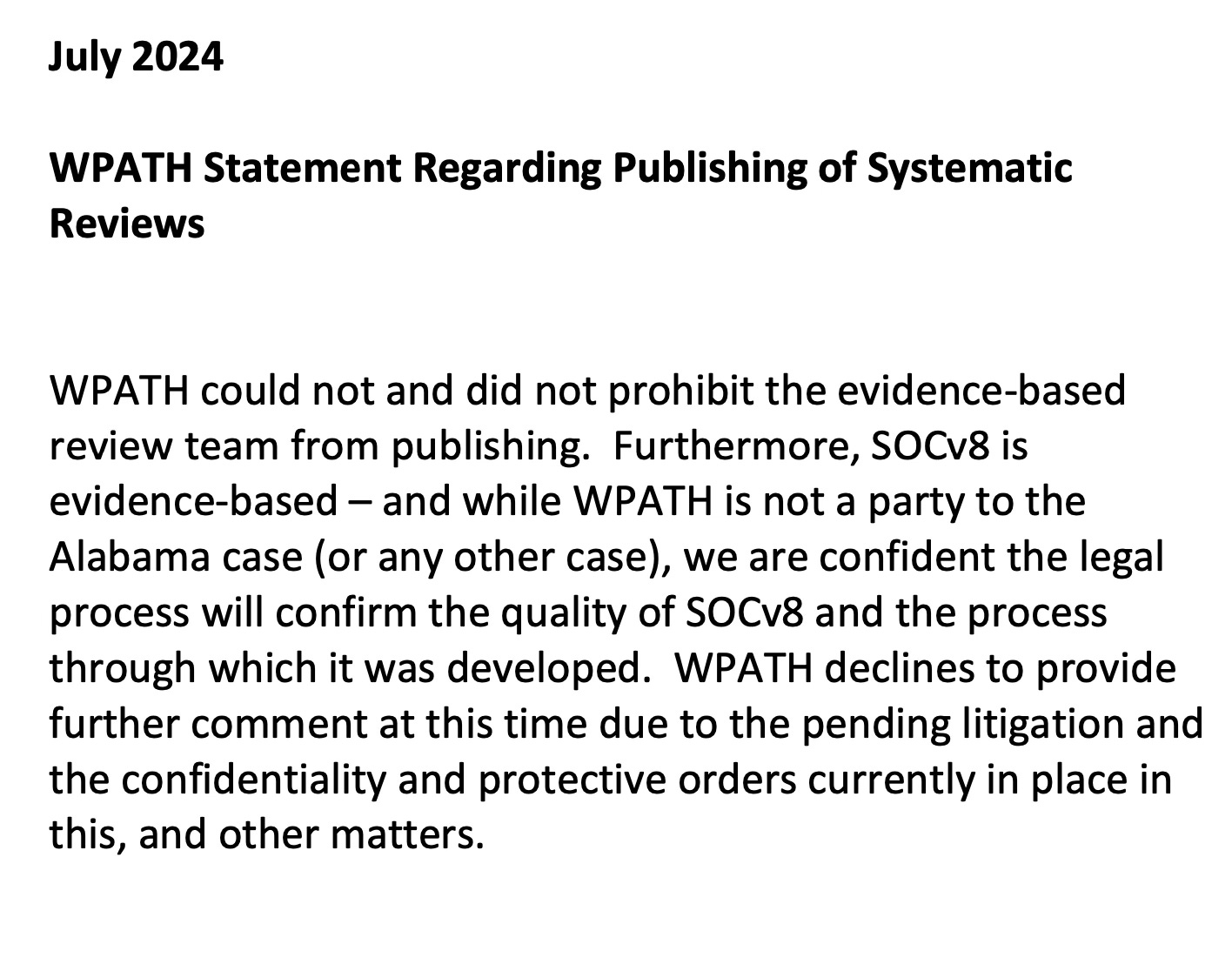
During the online video exchange, Dr. Williams also offered stinging criticism of the World Professional Association of Transgender Health—with Dr. Peters, who is both an ASPS and a WPATH member, at times nodding in agreement. The ASPS president addressed recent revelations that WPATH, which is a largely U.S.-based transgender medical-activist group that issues widely followed trans treatment guidelines, buried academic analyses that it had commissioned after the findings failed to portray gender-transition treatment in a sufficiently favorable light. Dr. Williams referred to WPATH’s handling of the matter as a “disaster” and criticized the beleaguered organization for a lack of transparency about data pertaining to gender-transition treatment.
“I'm not trying to come down on WPATH, but like, disaster, right? You know, the data is the data. And you have to put it forward.” —Dr. Steven Williams, president of the American Society of Plastic Surgeons
Such critical statements about pediatric gender medicine from Dr. Williams are remarkable, both in their unsparing candor and in the fact that such a prominent figure in the U.S. medical community would be willing to make them at all. His declarations about pediatric gender-transition treatment, both on Thursday and in a previous interview, have set ASPS apart from all the nation’s other major medical societies. Organizations such as the American Academy of Pediatrics (AAP) and the American Medical Association (AMA) have otherwise remained in lockstep in their support of minors’ access to gender-transition treatment and their opposition to state bans of such medical practices.
Here is the full audio of the Instagram Live between the two men:

A turning point in pediatric gender medicine
All this comes at a critical juncture in the young history of pediatric gender medicine. During its forthcoming term, the U.S. Supreme Court will consider whether Tennessee’s ban of pediatric gender-transition treatment, including the use of puberty blockers and cross-sex hormones to treat gender dysphoria in minors, is constitutional. To date, 24 states have passed bans on gender-transition treatment and surgeries for minors; two others have banned only such surgeries. Additionally, some two dozen medical-malpractice lawsuits have been filed against health and mental health providers—and, in on case, against the AAP—by people who underwent gender-transition treatment or surgeries as minors or young adults and later regretted it.
Even as many blue U.S. states have adopted policies protecting access to pediatric gender-transition treatment, recent systematic literature reviews—the gold standard of scientific evidence—have cast doubt on whether, given the current research base, such medical practices represent an ethical balance of risks versus benefits for minors. In April, Britain’s 388-page Cass Review, four years in the making, found such medical treatment was based on “remarkably weak evidence.” The U.K. subsequently joined four Scandinavian nations in sharply restricting access to puberty blockers and cross-sex hormones to treat gender dysphoria in those under the age of majority.


Dr. Peters, who goes by the moniker Queer Surgeon on social media and cuts a striking figure with his shock of perennially neon-pink hair, has established himself as a leading voice supporting access to gender-transition surgeries and treatment, in part through his unflappable social media presence. An assistant professor of surgery at Oregon Health & Science University in Portland, Dr. Peters maintains his position as a public figure in this field even in the face of virulent criticism. He has been subjected to pointed attacks, in particular, over his detailed descriptions of surgeries he performs for nonbinary-identifying patients that craft bodies unlike those found in nature—for example, a double mastectomy for a natal female that removes the nipples.
Peters pushes back against the Manhattan Institute
Dr. Peters was inspired to hold Thursday’s Instagram Live discussion with Dr. Williams after the ASPS issued a pair of public statements that publicly established the organization as the sole major U.S. medical society not to endorse pediatric gender-transition treatment. Additionally, Dr. Williams gave an interview to News Nation that ran on Sept. 2 in which he stated: “I don’t perform gender-affirming care in adolescents. And the reason why is because I don’t think the data supports it. So at my practice, we don’t even entertain that.”
In particular, Dr. Peters has been critical of how Leor Sapir, a fellow who researches pediatric gender medicine at the conservative think tank the Manhattan Institute, first reported the news of ASPS’s statement on pediatric gender medicine in an Aug. 12 article for City Journal with the headline: “A Consensus No Longer.”
Regarding U.S. medical societies’ ostensible consensus on supporting gender-transition treatment for minors, Mr. Sapir wrote:
[T]he U.S. consensus now appears to have its first big fracture. In July, the American Society of Plastic Surgeons, a major medical association representing 11,000 members and over 90 percent of the field in the U.S. and Canada, told me that it “has not endorsed any organization’s practice recommendations for the treatment of adolescents with gender dysphoria.” ASPS acknowledged that there is “considerable uncertainty as to the long-term efficacy for the use of chest and genital surgical interventions” and that “the existing evidence base is viewed as low quality/low certainty.”
…
Aware that WPATH suppressed systematic reviews of evidence while developing its latest “standards of care,” ASPS says that it “is reviewing and prioritizing several initiatives that best support evidence-based gender surgical care to provide guidance to plastic surgeons.” I also asked ASPS whether plastic surgeons share responsibility for determining the medical necessity of gender surgeries for minors. ASPS responded that surgeons are “members of the multidisciplinary care team” and as such “have a responsibility to provide comprehensive patient education and maintain a robust and evidence-based informed consent process, so patients and their families can set realistic expectations in the shared decision-making process.”
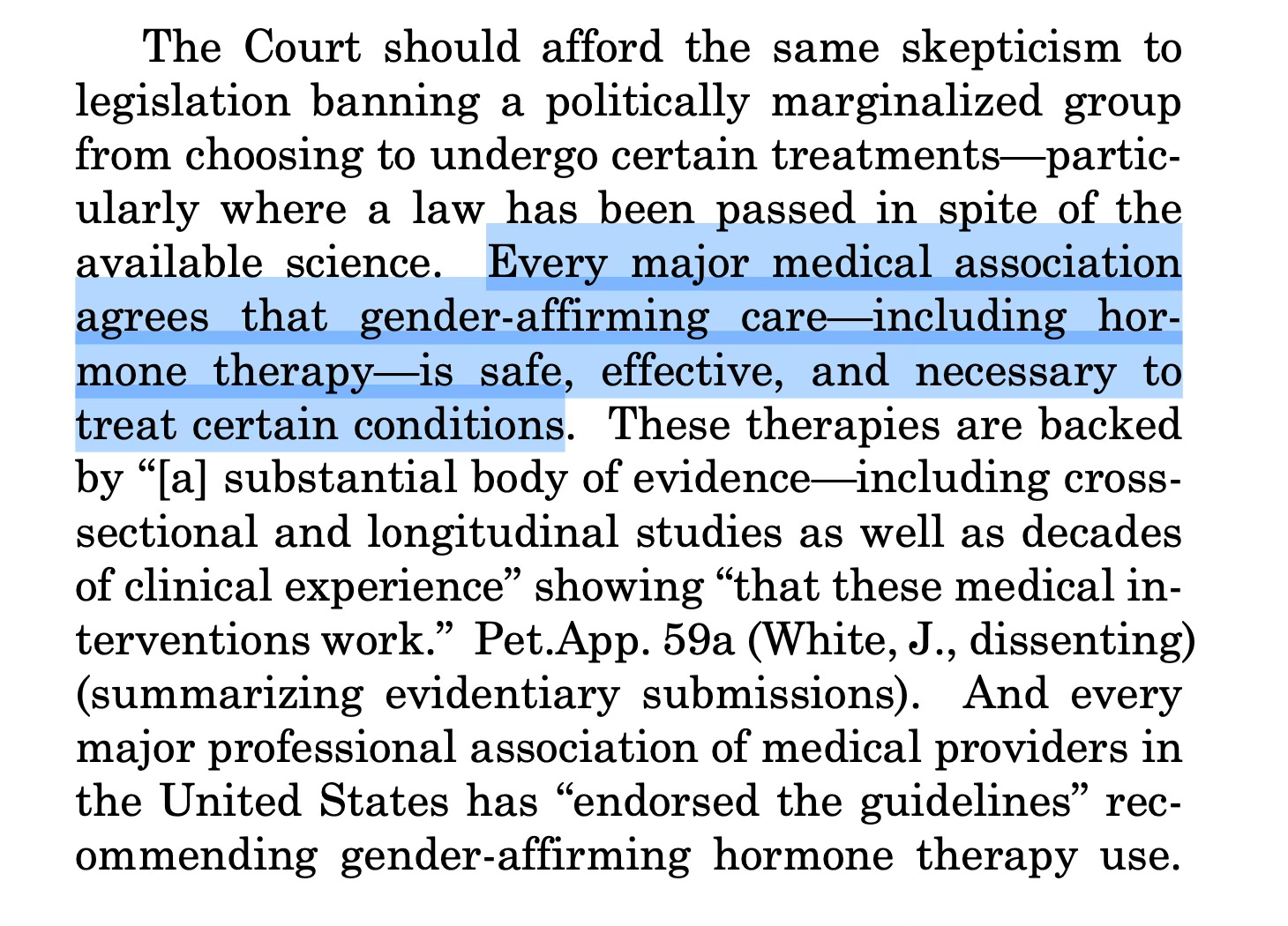
By providing Mr. Sapir with this statement, the ASPS cast a pall over a mantra that supporters of pediatric access to gender-transition treatment routinely leverage as a central defense against attacks of such medical practices: the notion that all major U.S. medical societies support these interventions. Notwithstanding the fact that this claim is now demonstrably false, some version of the mantra was included in a slew of amicus briefs submitted this week to the Supreme Court that urged the justices to find the Tennessee ban unconstitutional. Briefs that included the erroneous mantra were submitted by 164 members of Congress; 17 gender clinicians; actor Elliot Page and 56 other trans adults; the NAACP; the American Bar Association; the attorneys general of 19 blue states plus D.C.; and American Psychological Association and other mental health organizations.
After the City Journal report of the ASPS’s statement caused a media and social-media firestorm, the organization released a longer statement on Aug. 14. that added the following remarks:
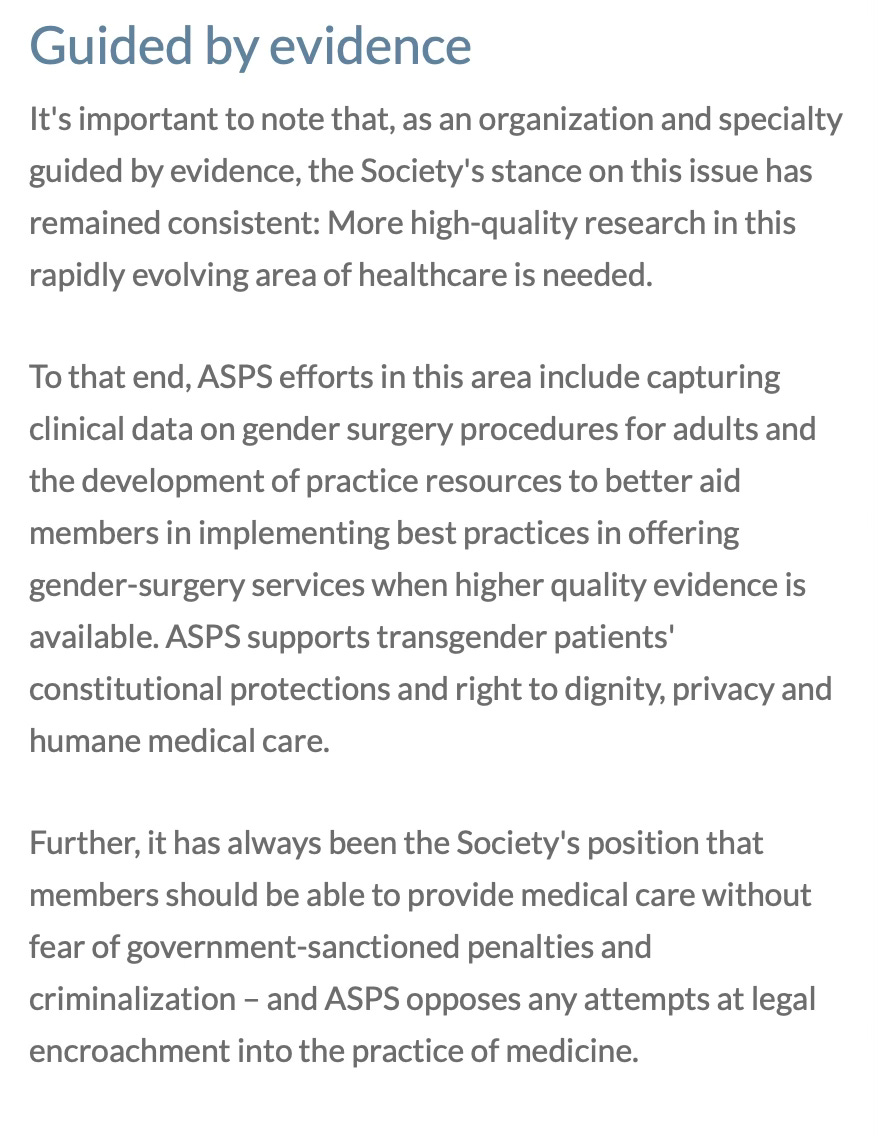
Guided by evidence
It's important to note that, as an organization and specialty guided by evidence, the Society’s stance on this issue has remained consistent: More high-quality research in this rapidly evolving area of healthcare is needed.
To that end, ASPS efforts in this area include capturing clinical data on gender surgery procedures for adults and the development of practice resources to better aid members in implementing best practices in offering gender-surgery services when higher quality evidence is available. ASPS supports transgender patients’ constitutional protections and right to dignity, privacy and humane medical care.
Further, it has always been the Society’s position that members should be able to provide medical care without fear of government-sanctioned penalties and criminalization – and ASPS opposes any attempts at legal encroachment into the practice of medicine.
In an Instagram video posted Aug. 15, Dr. Peters, inaccurately identifying Mr. Sapir as a journalist and denouncing him as an “anti-trans” messenger, claimed that the City Journal article had been false to claim that the ASPS was the first to “challenge the consensus” among U.S. medical groups over gender-affirming care for minors.
Similarly, activist-Substacker Erin Reed asserted in her Erin In The Morning newsletter on Aug. 16: “The ASPS has not altered its position on gender-affirming surgeries for minors for a simple reason: it has never issued any clinical practice guidelines for or against such care.”
Asserting that the ASPS’s statement opposed “government-sanctioned penalties and criminalization” of medical care, Dr. Peters further said on Instagram: “All that ASPS has said is that they’re continuing to evaluate the evidence in a field that is relatively new for young people—very reasonable and responsible.”
A crucial distinction, however, is that while the ASPS did not state that it opposed gender-transition treatment for minors, the organization did indeed state that it did not endorse such medical practices—specifically, it has “not endorsed any organization’s practice recommendations for the treatment of adolescents with gender dysphoria.” And while this lack of an endorsement may not have been publicly known before last month, it now officially common knowledge. This represents a profound shift in the public’s understanding of how the full swath of major U.S. medical societies consider this controversial and politically combustible issue.
Instagram Live: a tête-à-tête between surgeons
The hour-long exchange on Instagram Live on Sept. 5 between Dr. Peters and Dr. Williams was largely copacetic. And yet there was clear daylight between the two plastic surgeons as they debated the merits of conducting gender-transition surgeries on minors in a nascent medical field that is largely bereft of data to guide doctors.
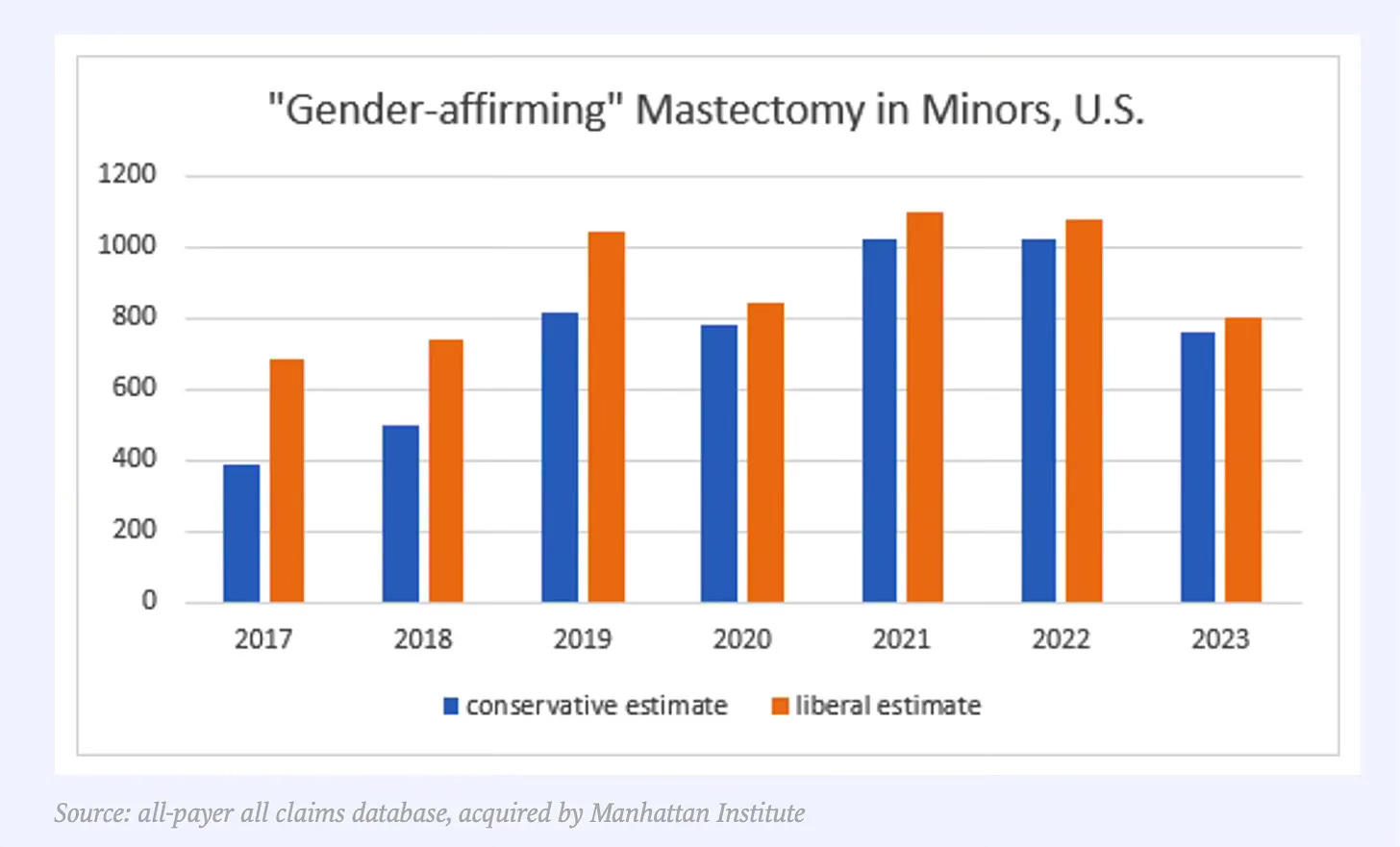
I recently reported on Mr. Sapir’s findings that an estimated 5,300 to 6,300 mastectomies, which comprise the overwhelming majority of pediatric gender-transition surgeries, were performed on gender dysphoric minors between 2017 and 2023. As I pointed out, Harvard recently misled the public about how common such surgeries are—falsely claiming they are “rarely performed,” and falsely suggesting they are vastly outweighed by gynecomastia operations among boys.

During the Instagram Live, Dr. Peters identified a contradiction in the position of conservative lawmakers regarding gender-transition surgeries for minors. Such lawmakers, he said, object to such practices on the grounds that they are lacking in sufficient supporting scientific data. And yet those same politicians advocate for bans on such surgeries, which only prevents researchers from collecting the necessary data to evaluate such practices. Dr. Peters advocated for allowing surgeons such as himself to continue performing gender-transition surgeries on gender-dysphoric minors so they can conduct the research he unreservedly agreed was greatly needed.
For his part, Dr. Williams cast doubt on the significance of his statement to News Nation indicating that he refuses to conduct such surgeries on children on principle. He said during the Instagram Live that he simply doesn’t perform any gender-transition surgeries, on children or adults; such operations are not within the scope of his practice. He was more than eager to agree with Dr. Peters that there is good evidence to support such operations for adults. And he was keen to delineate his support of adults’ right to access such surgeries from his and ASPS’s lack of support for pediatric access.
Dr. Williams lambastes WPATH
Dr. Williams praised Jesse Singal’s reporting for The Economist on WPATH’s fraught relationship with a team of evidence-based medicine experts at Johns Hopkins University. According to subpoenaed internal documents that were unsealed in June, WPATH contracted the Hopkins team to conduct a slew of systematic literature reviews about gender-transition treatment. But after findings from the reviews displeased WPATH, the organization sought to change the terms of their agreement with the researchers and wielded a heavy hand over what could be published. The vast majority of the analyses have consequently never seen the light of day.

“Not just WPATH, but all organizations have to be forthcoming with their data,” said Dr. Williams. “If there’s a reason they choose to exclude a certain amount of data, they have to be super transparent about that, and they have to explain it. Not just because there’s a particular agenda that one organization or one group or one political body wants, but because this is patient care we’re talking about.”
Regarding WPATH’s public comments about the Johns Hopkins reviews, Dr. Williams said: “I think WPATH has tried to have some answers. But personally, I don't think the answers have been satisfactory.”
Dr. Peters said of WPATH’s recent stumbles, “I think it took so much advocacy work for trans people even have the option to access care that all of these organizations are in that transition from advocacy based orientation or sorry organization to more legitimate scientific medical organization. And people need to allow that to happen.”
“But they need to hurry,” Dr. Williams replied. “I’m not trying to come down on WPATH,” “but like, disaster, right? You know: The data is the data. And you have to put it forward.”
WPATH, including is president, Dr. Marci Bowers, and the president of its U.S. division, Dr. Carl Streed, did not respond to my request for comment on Dr. Williams’ remarks.
Not in it for the money
Dr. Peters was adamant that he had no financial motivation to perform gender-transition surgeries.
“I don’t make money off of doing gender-affirming surgery,” he said. “I’m an employee at a public hospital, okay? Like, my colleagues that are like out in private practice, I assure you, are doing better than most of us in gender-affirming care.”
Dr. Bowers, however, recently disclosed in a sworn deposition for the litigation over Alabama’s ban on pediatric gender-transition treatment that her annual income from gender-transition surgeries, which she performs in private practice in Burlingame, California, exceeds $1 million. That figure is about double the average salary of a highly experienced Los Angeles plastic surgeon, according to Medscape. A trans woman, she is the first woman to have performed 2,000 vaginoplasties, according to her website.

Williams on the quality of the data for pediatric gender-transition treatment and on criminalization
During the Instagram Live, the two physicians engaged in a spirited discussion about the quality of the research backing gender-transition treatment and surgeries for minors. Dr. Williams went into even more precise detail about his reluctance to support such treatment in the pediatric context given the existing research base.
“This is a field that’s relatively new, and so the quality of evidence has to be really good before we’re going to advocate these types of procedures in adolescents,” Dr. Williams said. “ASPS will never advocate surgery for adolescent gender-affirming care until there’s better data.”
Dr. Williams recalled a question he received during a recent TV interview regarding gender-transition treatment for minors, saying, “And they said, ‘Well, what are you going to do when Trump bans this?’ I don’t know. Currently, ASPS doesn’t think that gender-affirming care for adolescents is appropriate.”
Then, referring to a hypothetical situation in which the data improved and supported the safety and efficacy of pediatric gender-transition treatment, Dr. Williams said: “If that data were to change, then I think we would have a problem with it”—meaning the ASPS would then oppose a ban of such treatment.
Seeking to pinpoint ASPS’s position on present-day bans, Dr. Peters referred to the segment of the organization’s recent statement that stressed it “supports transgender patients’ constitutional protections and right to dignity, privacy and humane medical care.”
“So to me,” Dr. Peters said in reference to this passage, “that categorically speaks against a blanket ban.”
“I’m not sure it speaks against a blanket ban,” Dr. Williams responded, indicating that the ASPS has not categorically opposed legislation banning pediatric gender-transition treatment. “I think this is where we may have a little bit of difference here, respectfully.”
Dr. Williams was adamant that he was opposed to lawmakers’ efforts to impose criminal penalties on doctors for providing gender-transition treatment to minors, as the laws that have been passed in some red states do. However, he left the door open for supporting non-criminalizing bans of such treatment—if new research were to emerge that suggested that such bans were, as he saw it, necessary.
“We’ve seen what criminalization looks like in terms of overall patient health: women, mortality when it comes to abortion,” Dr. Williams said. “Those types of things aren’t effective in terms of regulating health care. That’s not to say that if the data comes in and says—Oh my gosh, adolescent gender-affirming care is the worst thing ever, and we need to stop it!—there are ways that you could restrict that without criminalizing.”
Should such damning research findings about pediatric gender-transition treatment ever come to the fore, Dr. Peters said, “the physician groups providing it are going to be the first ones to raise the alarm and stop it.”
But Dr. Williams pointedly disagreed with Dr. Peters’ suggestion that physicians can necessarily be trusted, absent any and all state intervention, to self-correct in the event that they are providing egregiously harmful care.
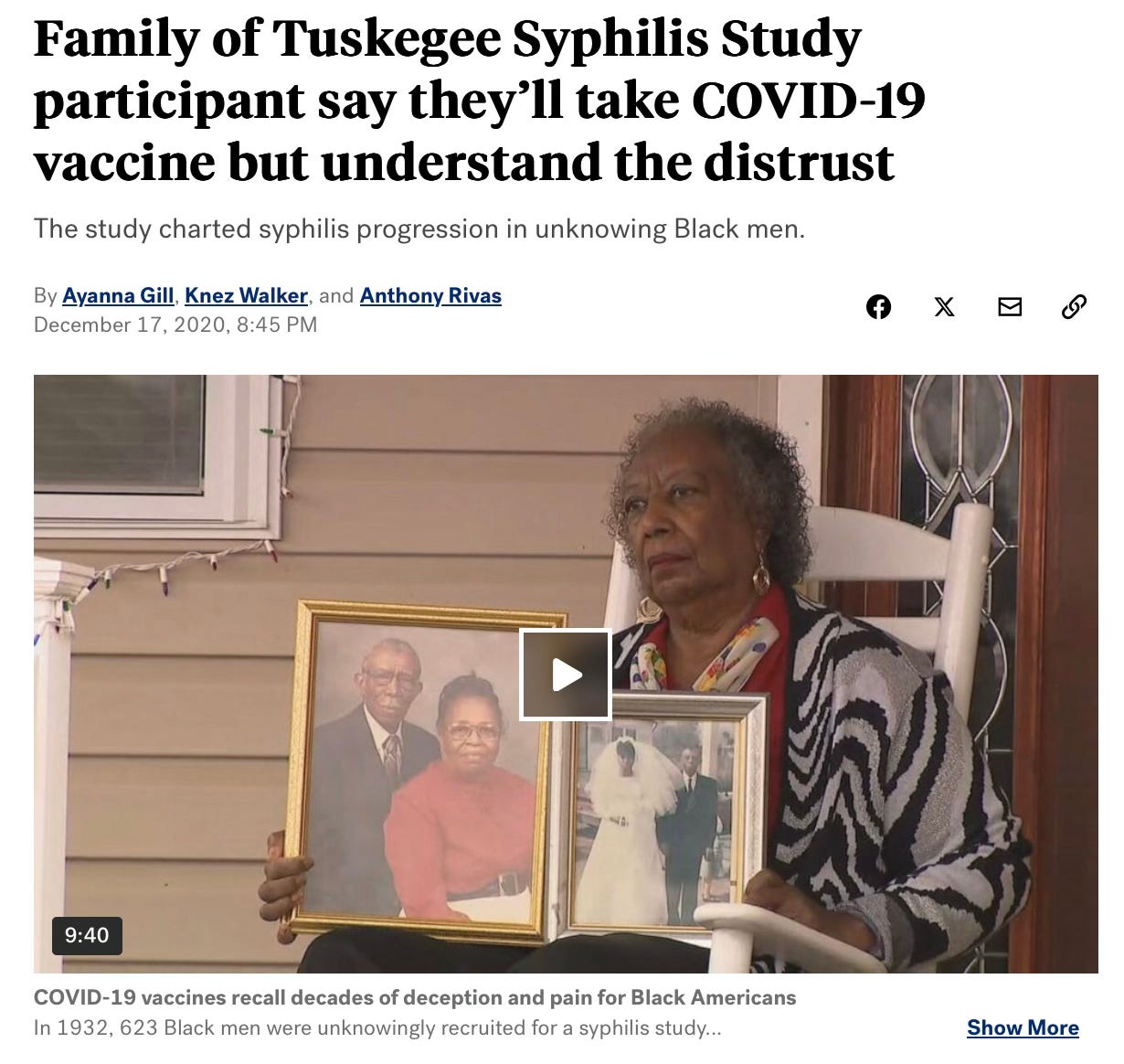
“Assuming that doctors always do the right things—that’s probably not the right assumption either,” Dr. Williams said. Then, referring to his own racial identity, he said: “In all honesty, again: Black man. So, you know, Tuskegee—Tuskegee experiments, those types of things. Those were doctors. They were doing terrible stuff.”
“Assuming that doctors always do the right things—that’s probably not the right assumption either.” —Dr. Steven Williams
In 1972, the American public learned that for the past 40 years, the U.S. Public Health Service, in partnership with the Tuskegee Institute, had studied the natural history of untreated syphilis among 400 Black men compared with 200 uninfected Black men. Those conducting the study never told these men that they had the potentially fatal infection or the true purpose of the study. Knowledge of this egregiously unethical and barbaric research has helped fuel medical mistrust among African Americans for the past half century, including regarding the Covid-19 vaccine.
Dr. Williams indicated that he saw a place for the state curtailing the practice of doctors if the health care field proved it could not self-regulate in a certain circumstances.
“I think that there has to be a balance,” Dr. Williams said. “It’s incredibly complicated, obviously.”
Wrapping up the conversation, Dr. Peters addressed the Instagram audience “However you’re coming into this or however you want to engage in this discussion, it should be informed by the evidence, not by personal or religious bias, including if you’re an expert in this field. And it should be based on the intent of actually wanting trans people to do well. That’s what we want at the end of the day. So much of the discourse is not based in that. And the humanity of people is really being overlooked here.”
“So you can think whatever you want to think,” Dr. Peters said. “But just remember, there’s people here at the end of the day.”
I am an independent journalist, specializing in science and health care coverage. I contribute to The New York Times, The Guardian, NBC News and The New York Sun. I have also written for the Washington Post, The Atlantic and The Nation.
Follow me on Twitter: @benryanwriter.
Visit my website: benryan.net
Thank you for your thorough work.
He played the oppression hierarchy uno-reverse card! So the white guy had to play along. Bravo!
On his own, Peters says things like "professionalism is transphobic".