

Dr. Jack Turban's Quietly Radical Bible On Pediatric Gender Medicine: a Primer
Dr. Jack Turban's Quietly Radical Bible On Pediatric Gender Medicine: a Primer
This is an appendix to my review for The New York Sun of the new book by UCSF child psychiatrist Dr. Jack Turban, "Free to Be: Understanding Kids & Gender Identity."

I just published a review in The New York Sun of the new book by University of California, San Francisco child psychiatrist Dr. Jack Turban, Free to Be: Understanding Kids & Gender Identity. This Substack is an appendix to my review (which I encourage you to read) in which I’ll provide supplementary passages from Turban’s book and other examples of Turban’s public discourse. (Please pardon my rather untidy highlighting and underlining in the images I’ve included of passages from the book.)
What Turban Says About the Evidence Base of Pediatric Gender-Transition Treatment
Turban writes in Free to Be that pediatric gender-affirming medical care, meaning providing puberty blockers and cross-sex hormones to minors to treat their gender-related distress, “isn’t experimental.” He cites “over a dozen studies” linking the use of these medications to “better mental health outcomes for adolescents.” In particular, he cites a prominent 2023 paper known as Chen et al.
From Free to Be, pp 225-226:
Gender-affirming medical care also isn’t experimental—over a dozen studies have linked treatments such as puberal suppression and gender-affirming hormones to better mental health outcomes for adolescents. Among them is a recent study of 315 adolescents with gender dysphoria, published in the prestigious New England Journal of Medicine, which found improvements in anxiety, depression, and life satisfaction after treatment.
Journalist Jesse Singal has thoroughly deconstructed (and one might say demolished) the Chen paper on his own Substack, finding: “The New, Highly Touted Study On Hormones For Transgender Teens Doesn’t Really Tell Us Much Of Anything.” The study, which followed adolescents treated for gender dysphoria for two years of cross-sex hormone use, identified only very minor shifts in mental health markers by the end of that time. Turban, however, touts that the study “found improvements in anxiety, depression and life satisfaction after treatment.” But in fact, as Singal notes, anxiety and depression only improved for transgender boys (biological females) and not for trans girls (natal boys).
Turban also does not acknowledge that two of the 315 participants in the Chen study died by suicide—and this was when they were being actively treated for gender dysphoria with hormones. That is an extraordinarily high death rate compared with other studies that have charted such a rate among gender-distressed youths.
Pediatric gender-transition treatment is widely touted by supporters of pediatric access to such drugs as “life saving,” despite a lack of evidence backing the claim that it mitigates suicide risk. (Turban does not claim in his book that gender-transition treatment prevents suicide death, but he does say it’s associated with a reduction in suicidality.)
As for Turban’s insistence that pediatric gender-transition treatment is not experimental, since 2020, the health authorities in five nations have reversed course on their policies for prescribing gender-transition treatment to children and have reclassified such treatment as, in fact, experimental. They have dramatically restricted access, in some cases to research settings only. These nations, which include the UK, Norway, Finland, Sweden and Denmark, made these changes in response to systematic literature reviews that found the evidence backing such treatment was wanting and inconclusive. (There is currently a political firestorm brewing in the UK over the fact that Parliament, following the National Health Service’s move in March to restrict puberty blocker access to clinical trials only, further banned private prescriptions of the drugs for gender-distressed minors.)

Turban also cites the 2022 Tordoff et al study of gender-transition treatment among youths. He states that it “found that mental health improvements from gender-affirming medical interventions could be separated out from the beneficial effects of psychotherapy.” What Turban does not mention is that among the youths in the Tordoff study who received gender-transition treatment, mental health markers did not change significantly during the 12-month study period. What did change was the composition of the untreated comparison group, which saw very high loss to follow-up. That comparison group, which only included data on seven youths at the 12-month mark, compared with 57 youths in the treatment group, had much poorer mental health by comparison.
And yet Turban uses causal language in his book to claim that this non-randomized study led to mental health improvements.
Jesse Singal has also thoroughly deconstructed Tordoff:
Turban’s Comments On Sexual-Dysfunction Risks of Treatment
When addressing the question of whether pediatric gender-transition treatment might cause sexual dysfunction, Turban cites the statement of one of the composite patients he uses to anchor his book’s narrative. This young trans woman (biological male) started puberty blockers at 12, by this point is on cross-sex hormones, has had a vaginoplasty (which surgically transforms the penis into what’s known as a neovagina) and is a thriving college student at Stanford. She cites “comments in the media” about such risks of sexual dysfunction and says that her own sexual function is good. Turban, who suggests that such concerns about sexual dysfunction are overblown, provides no supplemental commentary of his own in this passage about whether gender clinicians themselves also harbor such concerns.
And yet Dr. Marci Bowers, a gender-affirmation surgeon and president of the World Professional Association of Transgender Health, in a Zoom call (see below) told colleagues in the gender medicine field that there is a risk that trans girls (natal males) whose puberty is suppressed at Tanner Stage 2, or the first signs of puberty, and who go onto cross-sex hormones may never be able to have an orgasm.
British journalist Hannah Barnes writes in the new epilogue to her book Time to Think, which chronicles the collapse of the British pediatric gender clinic, GIDS, that Dutch researchers found troubling evidence of considerable sexual dysfunction among trans women whose puberty had been suppressed during adolescence.


Turban Suggests Doing Away With Psychosocial Assessments
At three key points in Free to Be, Turban strongly suggests that he thinks it would be better to do away with the psychosocial assessments that WPATH recommends prior to prescribing puberty blockers to gender-distressed children. He also hints that he thinks that these assessments should be done away with for prescribing cross-sex hormones as well.
All this is despite the fact that in his academic work, Turban has held up these assessments as a vital backbone of pediatric gender medicine. Last month, he took to X and denounced as “nonsense” New York Times columnist Pamela Paul’s assertion in a column that supporters of pediatric gender-transition treatment often denounce these assessments as “gatekeeping.” (Influential Canadian transfeminine jurist and activist Florence Ashley is perhaps the most prominent person to make such denunciations. See this 2019 paper of hers, for example.)
In the following section of Free to Be, Turban describes getting to know Dr. Michelle Forcier, who is one of the godmothers of pediatric gender medicine in the United States. Forcier, he recounts, told him how she believes that the use of the assessment protocols prior to prescribing puberty blockers is motivated by health care providers’ fear of malpractice suits waged by detransitioners, meaning people who have medically transitioned and then stopped taking hormones and gone back to identifying and presenting as their birth sex.



What Turban does not mention is that Forcier, along with her protégé Dr. Jason Rafferty, was herself named in just such a lawsuit late last year, which I have covered for The New York Sun. As I wrote:
Crucially, this suit also names as a defendant the American Academy of Pediatrics, the influential industry group that shapes best practices for medical treatment of children. The suit accuses the organization of engaging in a civil conspiracy with Dr. Rafferty and Dr. Forcier to develop, promote, and ultimately profit off what has become the prevailing American medical treatment model for pediatric gender care — a model that the suit alleges is based on a fraudulent and misleading representation of scientific research.
Forcier is also known, rather notoriously, as one of the pediatric gender medicine experts who were apparently duped into giving an interview to the incendiary conservative commentator and Daily Wire columnist Matt Walsh for his cheeky documentary, What Is a Woman? The interview proved embarrassing to Forcier when she responded to Walsh’s question about whether a chicken laying eggs is “assigned female” by saying, “Does a chicken have a gender identity? Does a chicken cry? Does a chicken commit suicide?”
In the following section of his book, Turban strongly suggests he thinks psychosocial evaluations for kids seeking gender-transition treatment are not beneficial and should be done away with, at least for puberty blockers. His colleagues, he suggests, agree: “Most in the field are now skeptical of this extra battery of assessments, as it’s unclear that all the hours of psychometrics by an additional psychologist are necessary, and this may carry the risk of further creating barriers to care and making young people feel stigmatized,” he writes, echoing Florence Ashley, whom he thanks in his acknowledgements.



In the following pages of Free to Be, Turban again cites the perspective of one of his composite patients, in this case a nonbinary adolescent who has opted not to receive gender-transition medications but who has OCD, for which Turban has just prescribed Prozac. The patient, Sam, says to him, “It’s funny that you could just talk about the side effects with us and prescribe [Prozac] instead of going through a whole series of therapy sessions the way my friends did for estrogen.” Turban then gives the strong impression that he agrees with the suggestion that cross-sex hormones should be as easy to get as Prozac for minors with gender dysphoria.



In a 2021 tweet, Turban went so far as to argue that puberty blockers, also known as GnRH analogs, should be available to gender-distressed minors without parental consent.

Turban’s suggestions in Free to Be that gatekeeping for pediatric gender-transition treatment should be discarded stand in sharp contrast to his recent academic and popular-press publishing, in which he has touted such assessments as important bedrocks of pediatric gender medicine.
In a July opinion essay in The New York Times, Turban wrote, citing his own recent paper on such assessments:
Among those who do have concerns with their physical sex characteristics, there is variation. For instance, many people have gender-related concerns about their chests, but not their genitals. Acknowledging this complexity, medical guidelines say it is essential for young people to have comprehensive mental health evaluations before initiating any gender-affirming medical intervention, to ensure their treatment team has a broad understanding of their gender identity experience and the best ways (both medical and nonmedical) to support them.
Below is a detailed bullet-point list Turban and his coauthors provide in their recent paper about what psychosocial assessments for gender-distressed minors can entail. Such an assessment, they write, is not meant to determine whether minor patients “‘are actually transgender,’ as many patients worry; rather this assessment is meant to help them understand the intricacies of pubertal suppression, so that they can make the best decision for themselves.”


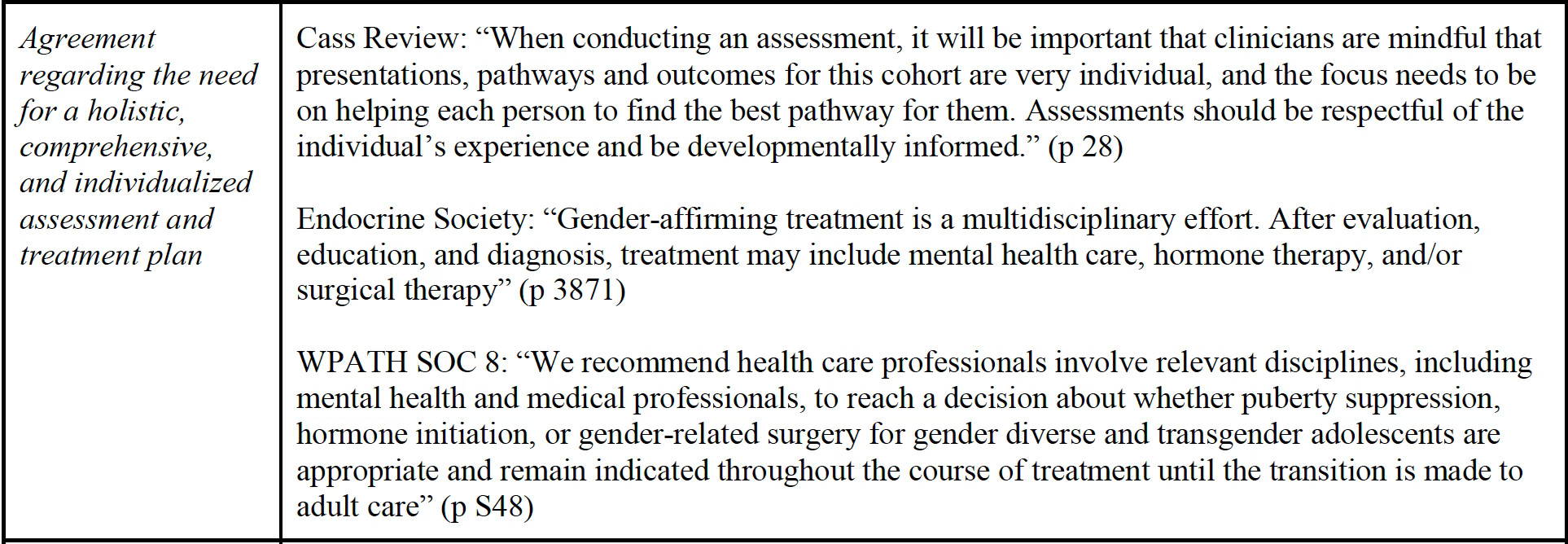
Finally, in a white paper Turban coauthored that criticizes the British Cass Review of pediatric gender medicine that Yale Law School put on its web site in July, Turban and his coauthors repeatedly stress the fundamental nature of psychosocial assessments in pediatric gender medicine:
If you found this Substack enlightening, kindly share my tweet thread about my review of Turban’s book.
Turban was on the Dr. Mike podcast for almost 2 hours. Most answers were “it’s complicated.” Every mention of studies discrediting his views was met with, “we have to look at the author and funding. They’re very biased against gender medicine.” Look in the mirror, dude.
Last week I renewed by paid subscription to this substack and for all the great work you do on X (twitter).
BTW, I noticed that political advocate Erin Reed did not mention on X the New York Times article exposing GLAAD's chief extravagant spending..........And didn't Reed recently get an award from them?
It's really amazing to me the degree of audience capture that some people have and how they seem to suffer 0 consequences for huge sins of omissions/commissions and outright lying.