


1 in 1,000 Privately Insured 17-Year-Olds Were Taking Cross-Sex Hormones Prior to State Bans
The authors of a new study analyzing 2018 to 2022 insurance claims data characterized such prescriptions as rare and said this rarity undermined arguments for bans of these interventions.


The video above is
an interview I did with the podcast Dollcast about this study.
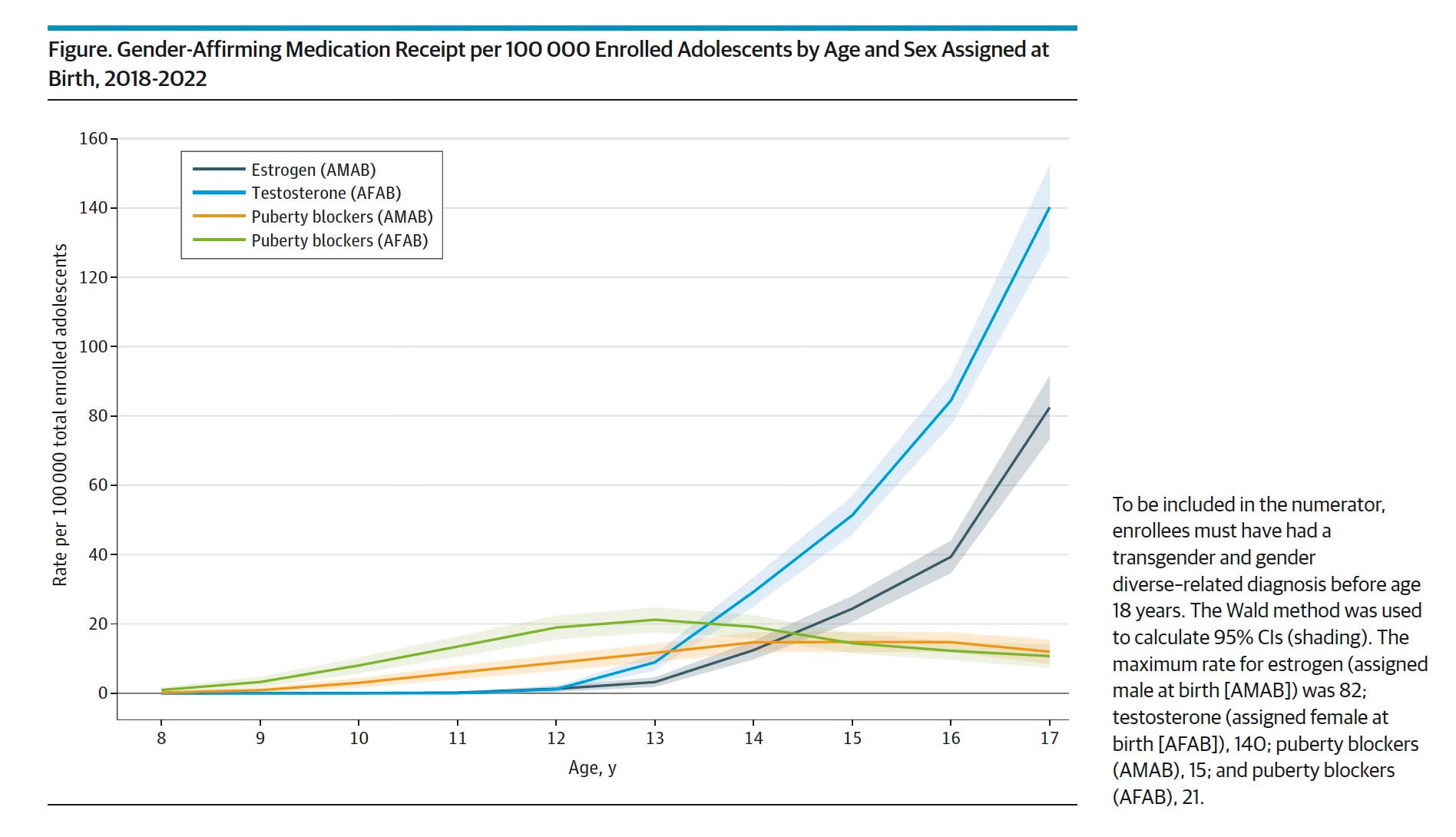
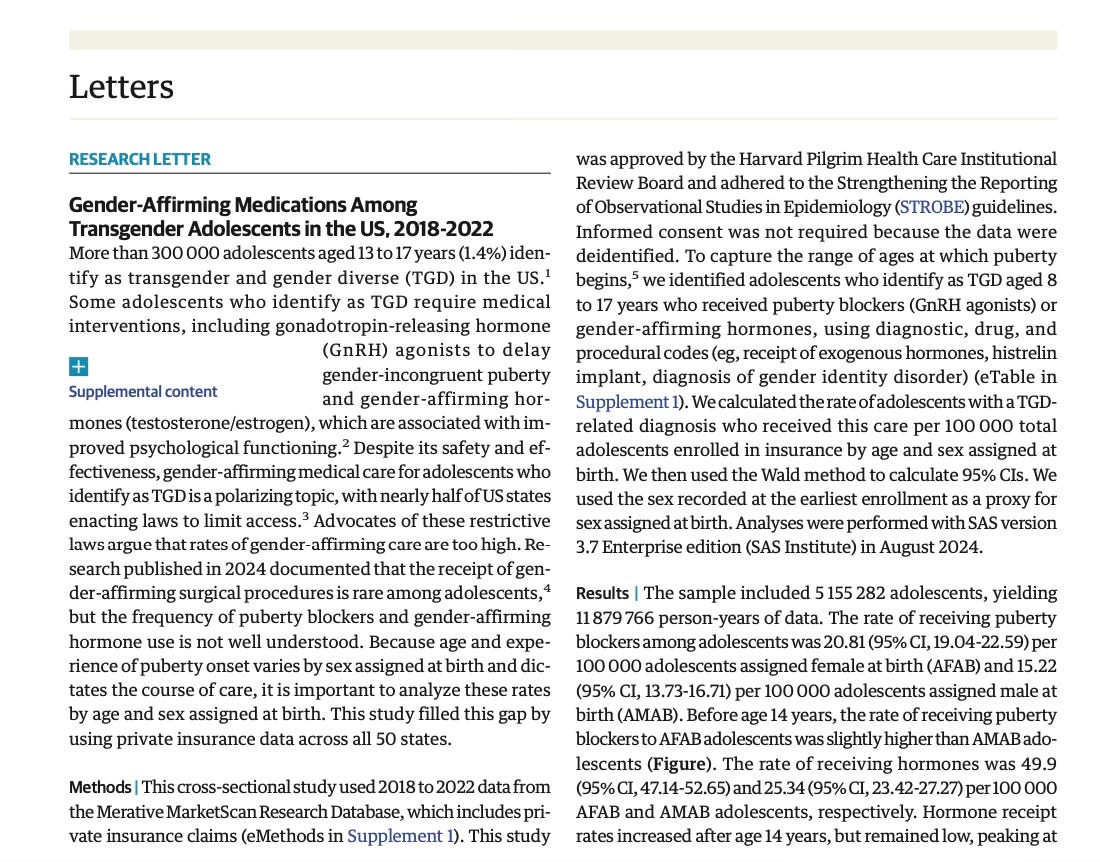
By age 17, about 1 in 1,000 privately insured minors were receiving gender-transition hormones between 2018 and 2022. This broke down to about 140 per 100,000 natal girls taking testosterone and 82 per 100,000 natal boys taking estrogen by this final year before teens hit the age of majority.
Compared with cross-sex hormones, puberty blockers were prescribed to adolescents with a transgender-related diagnosis at a much lower overall rate during this five-year period.
The authors of a new study reaching these findings characterized the prescription of gender-transition medications to adolescents under age 18—at an overall rate below 0.1%—as rare. Seeking to leverage their findings to score an advocacy win for the besieged field of pediatric gender medicine, they have argued that this rarity undermines arguments supporting state bans of such interventions for minors.
The investigators published their findings on Jan. 6 in a research letter in JAMA Pediatrics. The authors analyzed de-identified insurance-claims data from all 50 states regarding 5.2 million adolescents age 8 to 17 years old. This included a cumulative 11.9 million years of insurance-claims data.
The youngest children to have received cross-sex hormones, the study authors found, were 12 years old, albeit at a vanishingly low rate. The rate of such prescriptions rose through the adolescents’ teen years and peaked at age 17, with use consistently higher among natal girls.
The rate of puberty blocker use peaked at age 13 for natal girls, at about 20 per 100,000 females at this age, and age 16 for natal boys, at about 18 per 100,000 such males.
Such data are sorely needed to better understand the breadth of the pediatric gender medicine field amid the politicized upheaval over the prescribing of puberty blockers and cross-sex hormones to minors with gender dysphoria. (Gender dysphoria is a psychiatric diagnosis of marked distress stemming from a conflict between an individual’s gender identity and sex.) The period analyzed in the new study immediately predated the onset of an era that has seen the implementation of bans of such treatment in many states across the country.
The new study did not break down the prescription rates by year, only by biological sex and age. This oversight elides the steep recent increase—one that has been identified by other analyses—in the annual tally of gender-transition treatment prescriptions for adolescents, as well as a recent surge in diagnoses of gender dysphoria in young people.
Consequently, it is likely that gender-transition-drug prescription rates for minors were higher, perhaps much higher, in 2022 than in the across-the-board figures the new study reported regarding the five-year span that began in 2018.
This apparent fact went unmentioned by the research letter’s authors.
The study was conducted by investigators at the Harvard T.H. Chan School of Public Health, Harvard Pilgrim Health Care, and FOLX Health, which is a telehealth service that provides gender-transition treatments.
The authors noted that their findings are most generalizable to adolescents receiving health insurance through large-group plans. Other minors with gender dysphoria who have less comprehensive private coverage or Medicaid, or who are uninsured, presumably received puberty blockers and cross-sex hormones at lower rates, the investigators asserted.
Sorely needed data on gender-transition treatments for minors
The new study examined 2018 to 2022 data from the Merative MarketScan Research Database, which included claims data regarding people with private health insurance. The authors scoured the database for adolescents age 8 to 17 who had a transgender-related diagnosis and who received puberty blockers or cross-sex hormones.
The investigators broke down their data by age and natal sex, which they referred to as “sex-assigned at birth”—either “assigned male at birth,” or AMAB, or “assigned female at birth,” or AFAB.
(Note: I have been outspoken that such terms are scientifically inaccurate. With the exception of errors related to the approximately 1 in 5,500 infants who have differences in sexual development, aka intersex conditions, sex is, in fact, observed and documented at birth; it is not “assigned”. A simple glance at a baby’s external genitalia is 99.98% accurate at sexing an infant. Also, sex and gender identity are two different, if typically interrelated, things and should not be conflated in the context of transgender medical care.)
Overall, 21 out of 100,000—or 0.021% of—natal females age 8 to 17 received puberty blockers during the study period, as did 15 out of 100,000—or 0.015% of—natal males. As you can see from the chart above, this rate was slightly higher among natal females until the minors hit age 15.
And overall, 50 out of 100,000—or 0.05% of—adolescent natal girls received testosterone and 25 out of 100,000—or 0.025% of—natal boys received estrogen. The youngest age at which any child received cross-sex hormones was 12.
What notably goes unmentioned in the research letter
The research letter, which is considerably brief (journals typically have tight word-length caps), is compromised by a series of notable omissions.
In the letter’s discussion, the authors note: “The higher rates of puberty blocker and hormone receipt at younger ages among AFAB relative to AMAB adolescents aligns with their earlier onset of puberty and the current standards of care.” While natal females, of course, do hit puberty earlier, this only reference to the sex ratio in the data overlooks the very well documented fact that during the past decade, the sex ratio of children seeking care at pediatric gender clinics has flipped. Currently, a substantial majority of these minors are natal girls who only first began expressing a trans identity and openly expressing that they experience gender dysphoria following the onset of puberty.
As for the “current standards of care,” the World Professional Association for Transgender Health, or WPATH, quite notoriously caved to outside pressure from a Biden administration health official and the American Academy of Pediatrics and removed all age limits in the 2022 revision to its trans-care guidelines. So it is unclear what precisely the authors of the new research letter might have been referring to with the use of that phrase. The only tangentially age-based WPATH guideline related to gender-transition medications is that children cannot receive blockers until they hit the first signs of puberty. This typically occurs between age 8 and 13 for natal girls and age 9 and 14 for natal boys.
The investigators also did not apparently factor into their analysis prescriptions written under the diagnosis code “endocrine disorder not otherwise specified.” Health care providers have historically used this diagnosis at least some of the time when prescribing blockers or hormones to youth who identify as transgender. Thus, the omission of this code by the new study’s authors may also have artificially reduced the prescribing rate reported in the research letter.
The researchers also neglected to note that, according to other analyses, the annual rate of prescriptions for gender-transition treatment to minors surged during the study period. Given they did not break down their data by year, the new study’s authors are likely masking a higher rate of such prescriptions in 2022 in particular.
As I reported in October, a recent analysis of insurance-claims data by the nonprofit Do No Harm, which opposes pediatric gender-transition treatment, provided a conservative estimate indicating that between 2019 and 2023:
13,994 unique minors received gender-transition surgeries, treatment, or both.
5,747 minors received gender-transition surgeries.
8,579 minors received puberty blockers, cross-sex hormones, or both (the analysis did not disaggregate to show how many minors received each type of medication).

After examining Do No Harm’s data on the blue states that have no bans of such medical interventions, I reported that prescriptions for blockers and hormones universally surged in these states between 2019 and 2022. Then, in 2023, almost all such states saw at least a slight decline in prescriptions. This could have been the product of pent-up demand from during the Covid lockdowns ultimately being satisfied. Or it could have been a product of doctors becoming more cautious in their prescribing in the face of mounting political scrutiny and litigation, as well as parents becoming similarly reticent about consenting to such interventions for their children.

The authors of the Harvard research letter were keen to cite a recent study that also came out of the Chan School at the university finding that, in the words of the newer research letter, “the receipt of gender-affirming surgical procedures is rare among adolescents.”
I previously covered that study on surgeries and diagrammed how the opacity of its writing rendered its central finding woefully misleading. In addition to eliding the distinction between “breast reductions” and “top surgery,” aka a double mastectomy, the study relied on a considerably limited dataset with which to produce its figures.

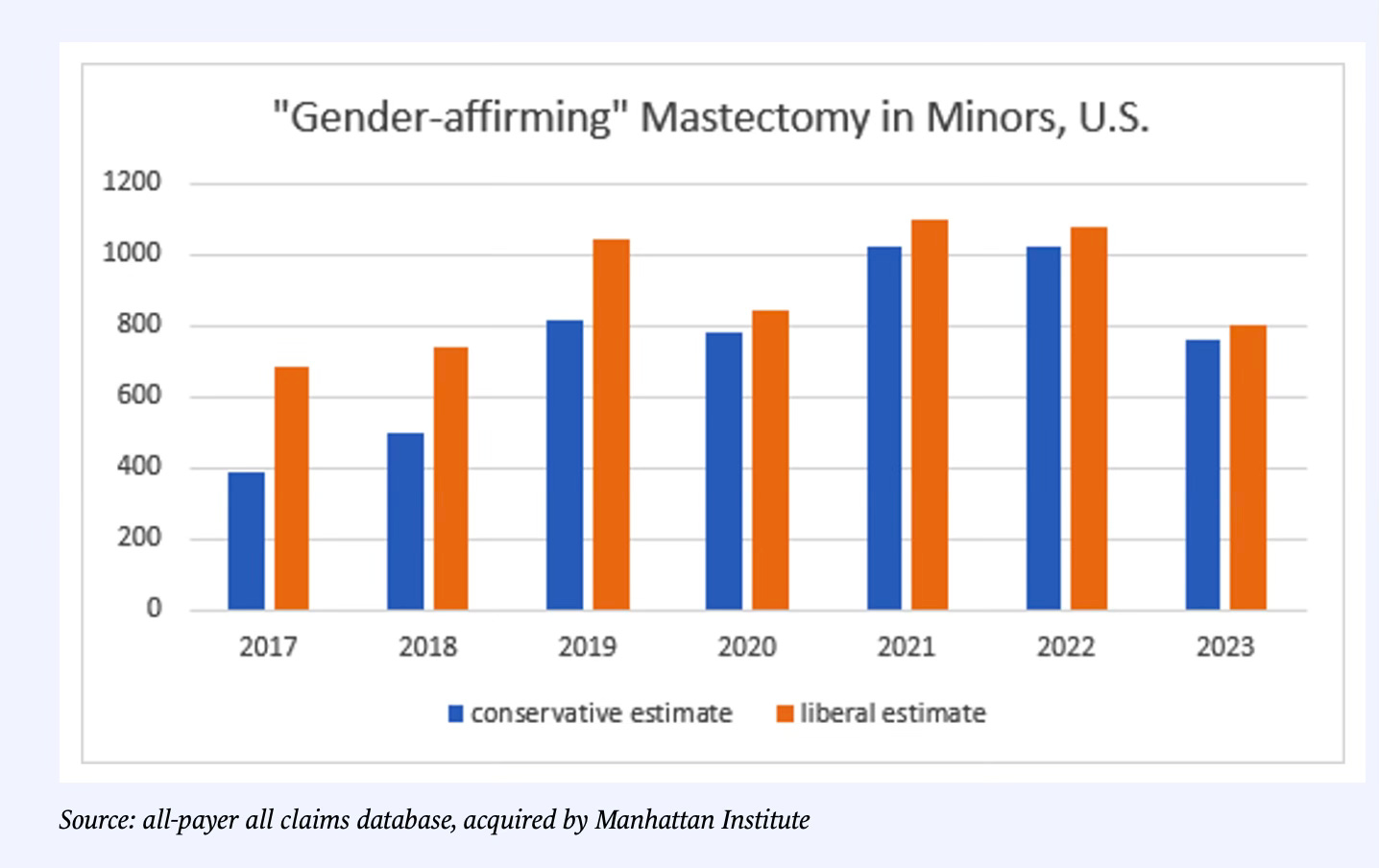
That particular group of Chan School authors identified just 85 gender-transition top surgeries among minors in 2019. But an analysis by Leor Sapir at the Manhattan Institute found that, in fact, by a conservative estimate, 5,288 to 6,294 natal girls received such surgeries between 2017 and 2023. Whether these figures still represent “rare” outcomes is, I suppose, a matter of opinion.
This chart diagrams the year-by-year top surgery rates:
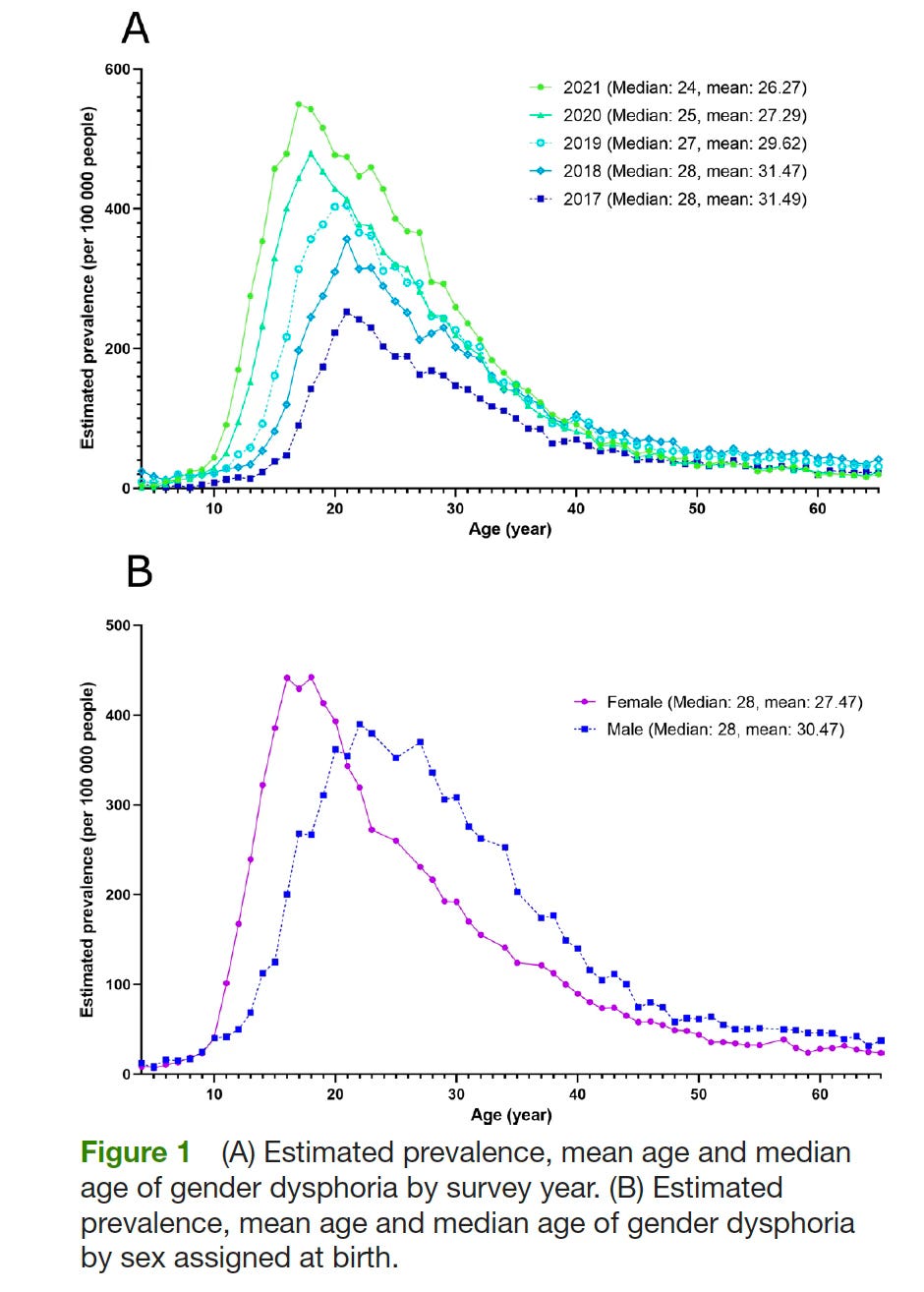
The authors of the new research letter on pediatric gender-transition treatment also did not mention that diagnoses of gender dysphoria both surged and skewed younger during their study period. According to a study of medical claims data published in the BMJ journal General Psychiatry in 2023, the average age at which people were diagnosed with gender dysphoria decreased from age 31 in 2017 to age 26 in 2021.
The first chart below diagrams the shift in the age at diagnosis and the rapid increase in such diagnoses. The second illustrates how, among minors, gender dysphoria diagnoses are much more common among natal girls compared with natal boys.
A distinct advocacy bent

The new research letter and the press release regarding the study that was blasted last week to science journalists under an embargo each had a distinct advocacy bent. The study authors were, as I noted, keen to leverage their findings of what they characterized as the rare prescription to minors of these gender-transition drugs to dispel what they decried as misinformation fueling state bans of such interventions.
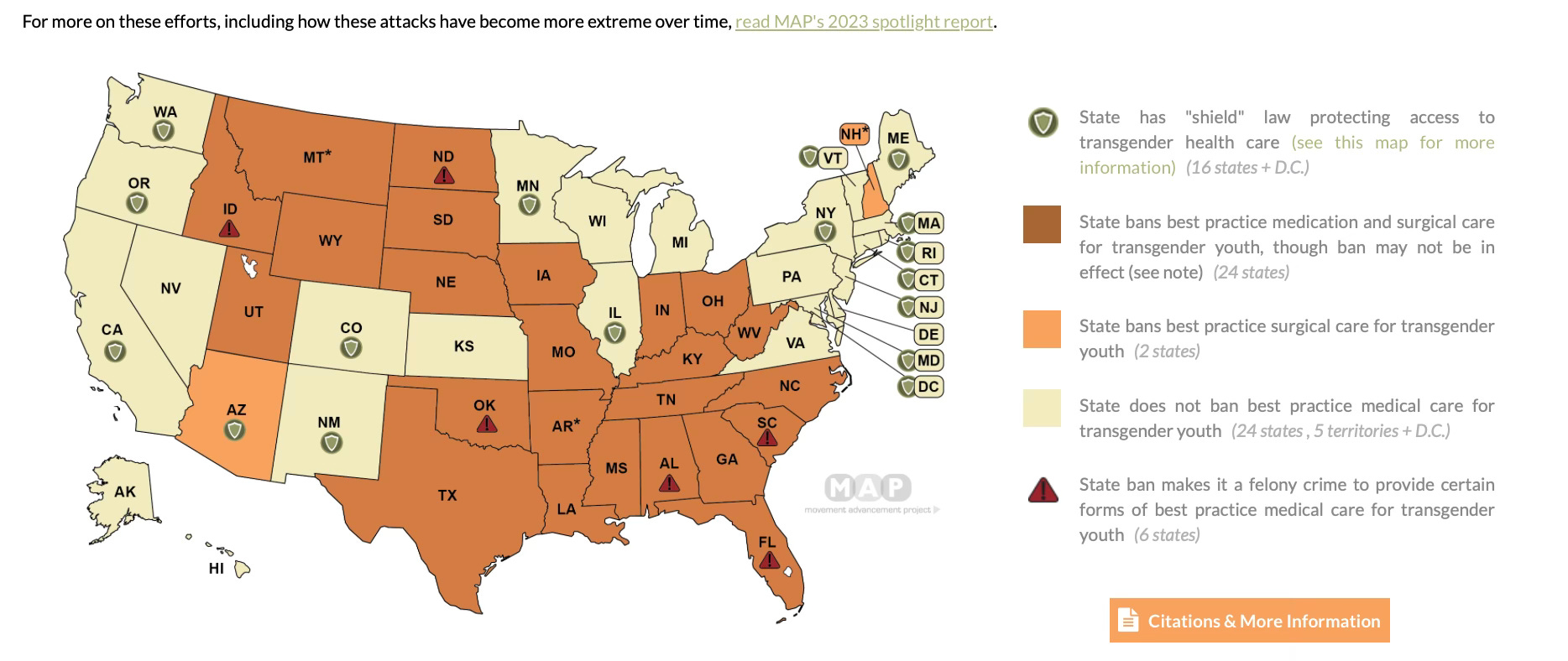
Since 2021, 24 states have banned puberty blockers, cross sex-hormones and surgeries for gender transitions among minors, and an additional two states have only banned such surgeries.
“Advocates of these restrictive laws argue that rates of gender-affirming care are too high,” the research letter stated.
In the associated press release, the study’s lead author, Landon Hughes, a post-doctoral fellow in epidemiology at the Chan School and Harvard Pilgrim’s LGBTQ Health Center of Excellence, additionally stated: “The politicization of gender-affirming care for transgender youth has been driven by a narrative that millions of children are using hormones and that this type of care is too freely given. Our findings reveal that is not the case.”
I am unaware of major backers or authors of such bans, or anyone with any credibility in this overall medical and political debate, issuing the false claim that millions of children are receiving drugs for this purpose. (If anyone can provide such an example, kindly make a note of it in the comments. It is always possible that Donald Trump, known for hyperbole, uttered such a claim. Update on Jan. 7: I figured out who it was: the Daily Wire’s Matt Walsh, on Joe Rogan, in Nov. 2022. And as I noted at the end of this Substack, Justice Sonya Sotomayor also recently made the same claim.) Such a figure would clearly be wildly erroneous, given that, according to a 2022 estimate by the Williams Institute at UCLA—a report cited by the Harvard research letter—perhaps 300,000, or 1.4%, of adolescents 13 to 17 years old identify as transgender.
Dr. Hughes did not return an email I sent to him on Friday with questions about his study.
The press release regarding the new research letter also included a comment from Jae Corman, a study coauthor and head of analytics and research at FOLX. Dr. Corman cited a more recent Centers for Disease Control and Prevention estimate that 3% of high school students identify as transgender. That still would put the number of teens identifying as trans under 1 million, but otherwise emphasizes that only a small fraction of minors expressing such an identity take blockers or hormones.
Dr. Hughes and his coauthors neglected to acknowledge that, rather than emphasizing the rate at which these treatments are prescribed, Republican lawmakers frequently center concerns about the safety of such medical interventions when rationalizing the bans. These politicians and other activists and medical experts who are critical of pediatric gender medicine also often cite the weakness of the supporting science, pointing, for example, to systematic literature reviews—the gold standard of scientific evidence—that have found such research wanting and inconclusive.
Take the ban passed by Tennessee lawmakers in 2023, called SB1, which the Supreme Court is now assessing to determine whether it violates the Equal Protection Clause of the Constitution. Justifications for the restrictions that were written into the bill included (I put certain key text in bold):
The legislature determines that medical procedures that alter a minor’s hormonal balance, remove a minor’s sex organs, or otherwise change a minor’s physical appearance are harmful to a minor when these medical procedures are performed for the purpose of enabling a minor to identify with, or live as, a purported identity inconsistent with the minor’s sex or treating purported discomfort or distress from a discordance between the minor’s sex and asserted identity. These procedures can lead to the minor becoming irreversibly sterile, having increased risk of disease and illness, or suffering from adverse and sometimes fatal psychological consequences. Moreover, the legislature finds it likely that not all harmful effects associated with these types of medical procedures when performed on a minor are yet fully known, as many of these procedures, when performed on a minor for such purposes, are experimental in nature and not supported by high-quality, long-term medical studies.
The text of the bill does not make any particular claims about the rate at which such treatments have been prescribed in Tennessee or elsewhere. But it does assert that these interventions have been provided to minors “with rapidly increasing frequency” in recent years. The bill also states that “minors lack the maturity to fully understand and appreciate the life-altering consequences of such procedures.”
As to Dr. Hughes’ assertion that claims that gender-transition drugs are “too freely given” are false, identifying the average rates of prescription of blockers and hormones across a five-year period cannot necessarily provide insights into the individual practices of pediatric gender clinics. Factors other than caution and so-called “gatekeeping,” such as insufficient staff in the face of surging demand, might otherwise limit prescribing.
As I recently reported for The New York Sun, it has been the policy since 2018 of Boston Children’s Hospital, the most prestigious such hospital in the nation, to provide gender dysphoric children and their parents only a single two-hour appointment with a psychologist to assess whether to refer a minor patient to endocrinology for a potential puberty blocker or cross-sex hormone prescription.

Additionally, a lawsuit filed last month against one of the top pediatric gender care doctors in the nation, Children’s Hospital Los Angeles’ Dr. Johanna Olson-Kennedy, revealed that she prescribed puberty blockers to a 12-year-old natal girl after a single appointment, with no assessment by a mental health professional. She then prescribed the girl, Clementine Breen, testosterone at 13 and referred her to receive a double mastectomy at 14. Ms. Breen, now 20, finally detransitioned at 19.

In a 2022 investigation, reporters for Reuters found seven pediatric gender clinics with a policy of permitting the prescribing gender-transition drugs to minors on the first appointment if the staff saw no “red flags.”
The new research letter also made a number of assertions about gender-transition treatment that are unsupported by evidence.
The letter stated that some adolescents who identify as trans “require” these medical interventions. As documents subpoenaed by the Alabama attorney general have indicated, WPATH inserted the term “medically necessary” throughout its guidelines on caring for trans adolescents despite knowing that the associated scientific research was weak and did not necessarily support such a declaration about the treatment’s necessity.
The research letter further stated that gender-transition treatment for minors is “associated with improved psychological functioning.” The citation for this statement is a paper known as Chen et al, which journalist Jesse Singal has thoroughly deconstructed as actually not demonstrating much in the way of psychological improvement among such young people. What’s more, the two-year study, of which Dr. Olson-Kennedy is a coauthor, had a strikingly high suicide death rate. Two of the 315 participants died by suicide. And this was among youth who were receiving the very medications that are so often touted as “life saving” by the very researchers who authored the paper.
Finally, the new research letter authors refer to gender-transition treatment’s “safety and effectiveness.” And yet a half-dozen systematic literature reviews have concluded that the efficacy of these treatments is essentially unknown.
As for safety, among natal males who start blockers early in puberty (at what is known as Tanner Stage 2) in particular, there is the substantial risk of infertility and sexual dysfunction should they continue on to take estrogen. (Virtually all minors who start puberty blockers to treat gender dysphoria later take cross-sex hormones.) Of the original group of 55 minors who underwent this treatment in the Netherlands beginning in the mid-1990s and whose cases were written up in a landmark paper in 2014 that helped give rise to the global pediatric gender medicine field, one participant died from complications related to a vaginoplasty.
Below is a video of Dr. Marci Bowers, a prominent gender-transition surgeon who recently completed her term as president of WPATH, outlining her concerns about sexual dysfunction in natal males who begin gender-transition treatment during early adolescence. You can see Dr. Olson-Kennedy in the video and note that Dr. Bowers refers to her (as “Jo”).
Above all, the new research letter speaks to a paradox in the debate over pediatric gender transition treatment. Supporters of these interventions often point to the low numbers of children receiving them as a defense against bans. While on the other hand, many of these same supporters also often decry the lengthy waiting lists at pediatric gender clinics, indicating that they wish that many more children were able to access drugs that they tout as safe and effective at treating gender dysphoria.
Most strikingly, in April, in a letter lashing out against Britain’s Cass Review, the four-year effort to analyze the pediatric gender-medicine field that concluded it was based on “remarkably weak evidence,” WPATH went so far as to assert that the majority of adolescents identifying as transgender would do better to receive gender-transition treatment.
That would comprise at least 150,000 teenage minors, or 1.5% of this cohort, receiving these medications in any given year and at least 30,000 of them turning 18 annually.
Update (Jan. 7): I did find someone who falsely claimed that “millions” of children receive gender-transition treatment. But it was not from a conservative seeking to attack minors’ access to such interventions. It was Justice Sonya Sotomayor, who during the oral arguments at the Supreme Court on Dec. 4 over the Skrmetti case, said: “So the question in my mind is not do policymakers decide whether one person's life is more valuable than the millions of others who get relief from this treatment? The question is: Can you stop one sex from the other --one person of one sex from another sex from receiving that benefit?”
I should’ve remembered, since I was there, after all.

Here is the full research note, which I gather has a paywall:
I am an independent journalist, specializing in science and health care coverage. I contribute to The New York Times, The Guardian, NBC News and The New York Sun. I have also written for theWashington Post, The Atlantic and The Nation. Follow me on Twitter: @benryanwriter and Bluesky: @benryanwriter.bsky.social. Visit my website: benryan.net
The moral relativism in this study is astounding. It's like saying the Manson Family deserved to go free because they only harmed a small percentage of the population of California. And of course we have no numbers for the drugs obtained from online grey-market and illegal sources which cannot be claimed on health insurance.
A 2015 systematic review (https://www.sciencedirect.com/science/article/pii/S0924933815000917) whose authors include Jon Arcelus and Walter Bouman (the latter is a past president and a current member of the Executive Committee of WPATH, and both Arcelus and Bouman are coauthors of WPATH's SOC 8) arrived at a meta-estimate of 0.0046% (or 4.6 per 100,000): 0.0068% being trans women and 0.0026% trans men (the ratio of 2.6:1 between the two is consistent with the historical preponderance of transwomen). That number - 0.0046% - is about 22 times larger than the 0.1% that these researchers are claiming as "rare."
Numbers like those presented in the 2015 systematic review are not outliers either. A 2019 narrative review found five different ways of classifying transgender and nonbinary (TGNB) population estimates across 43 studies conducted in various locations at different times. This narrative review, all of whose six authors share authorship of WPATH’s SOC8 (including the SOC8’s lead author, Eli Coleman), was subsequently cited by Baker et al. (2021) - the WPATH-commissioned systematic review on the mental health benefits of hormones (https://academic.oup.com/jes/article/5/4/bvab011/6126016). In their systematic review, Baker et al. distinguished between studies that “rely on clinical records” and those that “focus… on self-report among nonclinical populations" (p. 2).
Other researchers who studied the size of the transgender population have also highlighted this distinction. For example, one systematic review (of 27 studies) from 2016 (https://academic.oup.com/jsm/article/13/4/613/6940166) stressed “the importance of adhering to specific case definitions [“transgender-related diagnoses” and “self-reported transgender identity”] because the results can range by orders of magnitude” (p. 13). Specifically, its estimate for “self-reported transgender identity” among adults (0.871%) was 128 times larger than the estimate for “transgender-related diagnoses” (0.0068%).
The 2019 narrative review (mentioned above) found that the median estimate of those who received or requested medical interventions in countries as varied as the United States, Italy, Serbia, Netherlands, Belgium, Sweden, Spain, and Singapore between 1968-2011 is 0.00526%. Remember, this is a review authored by WPATH SOC8 writers and approved by WPATH's systematic review on the mental health outcomes from cross-sex hormones.
Claiming 0.1% to be "rare" even when there are several reviews within the last 10 years - authored by the doyens of WPATH, no less - that show that the actual numbers are orders of magnitude smaller, is the height of chutzpah. For every minor who might have qualified for medical interventions less than 10 years back, 21 more are being given these medications. On the basis of what evidence? That of Johanna Olson Kennedy, who did not publish her findings about puberty blockers, or published findings about hormones after changing the study protocol wholesale, one that Jesse Singal had to spend two giant posts (the first one here: https://jessesingal.substack.com/p/on-scientific-transparency-researcher) to find all its shortcomings?