
How Common Is Detransitioning?
Never trust someone who says they know precisely how commonly people detransition. Research on the subject, especially pertaining to minors, remains maddeningly hazy.


If anything is clear about the profoundly messy and politicized subject of detransitioning, one should never trust someone if they claim to have clarity on precisely how common this phenomenon is.
The correct answer is: “We’re not sure.”
More specifically, the available research on the prevalence of detransitioning provides a general sense that at most, a fraction of people who medically transition genders ultimately cease treatment with cross-sex hormones. How small that fraction is, and what proportion of those who discontinue hormone treatment actually revert to presenting and identifying as their birth sex, and what proportion regret having transitioned in the first place, remains hazy.
The detransitioning rate is especially unclear among those who underwent gender-transition treatment as minors, including with puberty blockers, cross-sex hormones and sometimes surgeries (a double mastectomy is by far the most common such operation in minors with gender dysphoria). With a couple of notable exceptions, the follow-up in studies that have published detransitioning rates has been woefully inadequate—usually no more than 12 to 24 months.

“Some professionals have referred to this [12- to 24-month] interval as the ‘honeymoon period,’ which may not be a realistic representation of the trajectories of individuals who medically transition,” wrote the authors of a review of the literature on detransitioning that was published in 2023.
Overall, studies of detransitioning are also hampered by high loss to follow-up among members of the cohorts who have received medicalized gender transition interventions, hitting 30% to 40% in some studies. Physician-researcher Dr. Lisa Littman has found that many people who detransition do not inform their former care providers about having done so, leaving a major blind spot.
Two of the most valuable data sets about pediatric gender transition, from gender clinics in Australia and the UK, have cut-offs once the youth turn 18. Studies of detransition among these youth are based on data from youth’s discharge from pediatric gender clinics. This prevents us from determining whether such individuals detransitioned during young adulthood.
The need for such long-term follow-up data is crucial. Kinnon Ross MacKinnon of York University is the most prominent researcher to study detransitioning; in particular, he examines the varied, nuanced and complex reasons why people detransition. In a recent AMA Journal of Ethics interview, Dr. MacKinnon said that detransitioning can take four to eight years. Similarly, Britain’s Cass Review stated that “the Review has heard from a number of clinicians working in adult gender services that the time to detransition ranges from 5-10 years, so follow-up intervals on studies on medical treatment are too short to capture this.”
Unfortunately, the UK National Health Service’s adult gender clinics refused to share de-identified data regarding former patients of the NHS’s now-shuttered pediatric gender clinic, the Gender Identity Development Service, or GIDS. Such data could have shed important light on the long-term outcomes of adults who received gender-transition drugs as minors and have since attended an adult gender clinic.
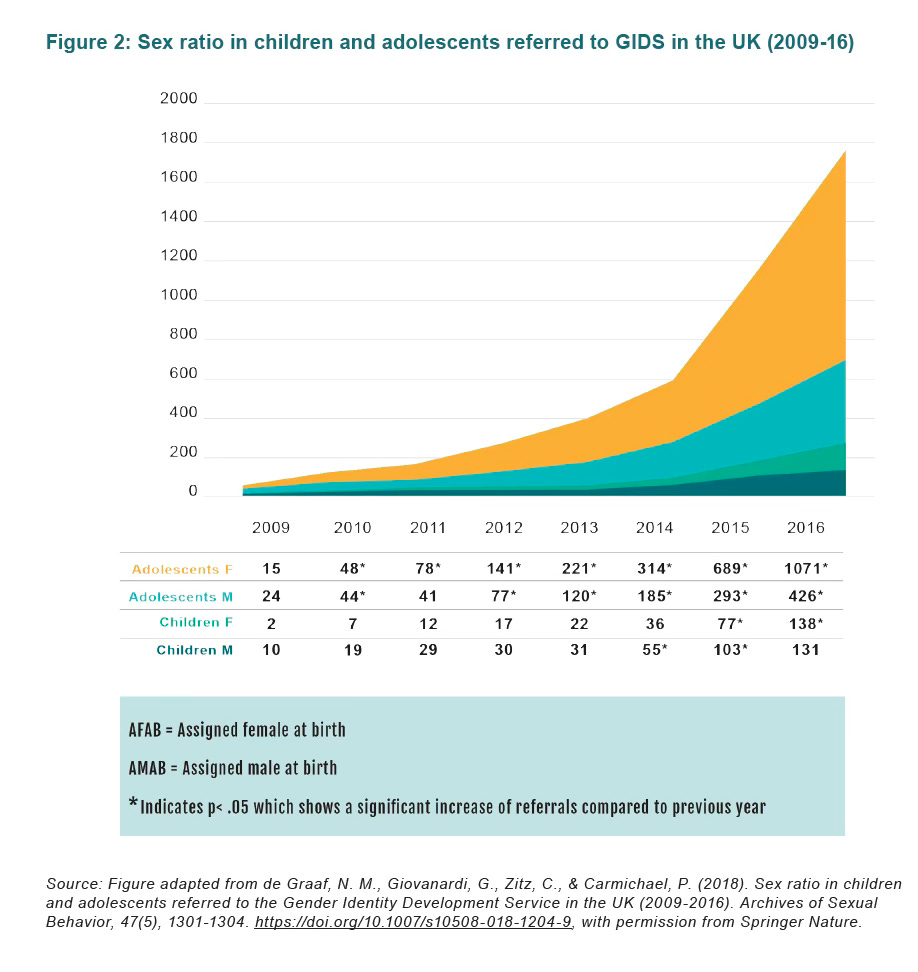
Researchers’ ability to understand the prevalence of detransitioning among those who received cross-sex hormones as minors is further hampered by how dramatically the cohort of youths with gender dysphoria has changed since in the early 2010s. Staring in about 2012 to 2014, gender clinics across the Western world began to see a surge in patients who were natal females, who only first began expressing cross-sex identification and gender dysphoria after puberty’s onset, who had a high rate of psychiatric conditions in addition to gender dysphoria, and who had a high rate of autism spectrum disorders. This new predominant phenotype stood in sharp contrast to the typical pediatric gender clinic patient dating back to the 1990s: a natal boy who first began expressing gender dysphoria in early childhood.
Not enough time has passed to properly assess the long-term outcomes of this new cohort of young people who have received testosterone treatment during adolescence. Plus, there is not enough research being conducted about this new cohort in the first place. Such efforts will now be hampered even further by the Trump administration’s all-out assault on federally funded research about transgender populations.
Another central problem in the effort to understand detransitioning is a lack of uniform and precise definitions across the research field of term “detransition” and of the notion of “regret” associated with having medically transitioned.
It appears that the World Professional Association for Transgender Health (WPATH) has shirked its responsibility to promote consensus on such terms so that they can be applied uniformly across research projects. Nor has WPATH promoted such research—quite the contrary.
The imperative to study detransitioning is also impeded by fears among gender-medicine researchers, which are certainly not unfounded, that doing so will produce results that will be leveraged by the right wing in an effort to undermine this field of medicine.
I conferred with Erica Anderson, a psychologist and former head of WPATH’s U.S. branch, USPATH. She told me that WPATH has not to her knowledge ever sought to define the terms “detransitioning” and “regret” and to promote research on the subject. On the contrary, Dr. Anderson told me, “WPATH has criticized those of us raising questions” about detransitioning and “calling for compassion” for detransitioners.
“WPATH leadership maintained that detransition was rare, and further that it was more important to advocate for trans people getting what they need,” Dr. Anderson said.
She added that the two most prominent researchers to investigate detransitioning, Dr. Littman and Dr. MacKinnon, have “both been reviled by the” trans-rights activists “for their attempts to understand aspects of this. WPATH piled on repeatedly.”
I recommend you check out Dr. MacKinnon’s Substack:

Dr. MacKinnon noted in his recent podcast that about one-third to 60% of detransitioning involves some form of regret.
Multiple studies have criticized right-wing opponents of pediatric gender-transition treatment in particular for weaponizing detransitioning and for presuming that all such discontinuation of these medical interventions is based in regret.
But Dr. MacKinnon’s research has found that detransitioning is also often driven by external factors, such as pressure from family, financial reasons, or not being able to pass as the opposite sex.
In a recent paper outlining how he has established his research cohort of 957 detransitioners (which required clever weeding out of bad actors and fraudulent responses submitted by people looking to foil his research), Dr. MacKinnon noted that studies published in Western nations estimate that between 1% and 13.1% of transgender people experience detransitioning at some point. “However,” he wrote, “due to study designs, it can be difficult to know the extent to which stopping treatments or detransition is temporary or permanent.”
So let’s take a closer look at what the available research does tell use about how common detransitioning is.
A new systematic review of detransitioning statistics
Dr. Eva Feigerlova, who is on the faculty of medicine at CUESim in Lorriane, France, in March published in The Journal of Sexual Medicine a systematic review of research regarding both minors and adults who received gender-transition treatment. She sought to assess what the available published literature tells us about how common detransitioning is.
The review included 15 observational studies, published between 2014 and May 2024, that between them included 3,804 minors and 3,270 adults. Ten of the studies included children and adolescents and five included adults. The studies were published in Western Europe, the United States and Australia.
Among children who started puberty blockers:
1.6% to 7.6% stopped taking blockers, including 1% to 3.8% who did so because they did not wish to pursue a gender transition.
Two studies that reported on reidentification with natal sex found that 0.4% to 5.3% of children who took puberty blockers did so.
Among people who started cross-sex hormones as minors:
The rate of cross-sex hormone discontinuation typically ranged from 1.5% to 2.4%.
However, a pair of studies, published in 2022 and 2023, analyzing the first 20 years of the Dutch protocol (which first established pediatric gender medicine) in Amsterdam found a pooled detransition rate of 3.2%.
Among both adults and adolescents who received cross-sex hormones:
Discontinuation rates ranged from 1.6% to 9.8%, including 0.5% to 9.8% among those who no longer wished to continue with a gender transition.
However, there were studies that reported discontinuation rates far outside this general range. This included one 2022 study out of Denmark that analyzed national medical data covering 2000 to 2018 and reported a discontinuation rate of 0.06% per year among those who took cross-sex hormones.
Another frequently cited study, published in 2022, looked at 2009 to 2018 medical and pharmacy records from the US Military Healthcare System of 952 people who started cross-sex hormones. It found that treatment discontinuation rates after four years of follow-up were 19% among natal males who took estrogen and 35.6% among natal females who took testosterone. Among those who started treatment as minors, the four-year discontinuation rate was higher among those who started as minors, at 25.6% compared with those who started after turning 18, at 35.6%.
Because this military study was a chart review, it remains unknown why these people stopped taking hormones.
Among all the studies analyzed, the available reasons people expressed for discontinuing cross-sex hormone treatment were varied. They included no longer identifying as transgender, meeting treatment goals, side effects, and financial or social issues.
The quality of detransitioning research is poor
Dr. Feigerlova was quite critical of the research she analyzed. She concluded that the “overall quality of the included studies was low, meaning we can hold little confidence that their findings are reflective of real world phenomena. The studies varied in how authors defined detransition, and it was not clear whether individuals identified as nonbinary were excluded.”
She further stated that “most of the studies were retrospective and unblinded,” and most had study populations that were too small to yield statistically significant findings about detransition rates.
Dr. Feigerlova concluded that detransition among those who have received gender-transition treatments “has been insufficiently investigated, highlighting the need for long-term follow-up in studies.”
She did not include surveys of online communities in her analysis, because, she wrote, “they are susceptible to self-selection and nonresponse bias.” This includes a rather notorious 2021 paper by University of California, San Francisco child psychiatrist Dr. Jack Turban, which relied on respondents to the U.S. Transgender Survey to analyze factors leading to detransition. The paper makes little of the fact that the people who responded to the survey had to currently identify as transgender, meaning that the 13.1% who reported a history of detransitioning all likely then retransitioned in some form. And yet this paper is often highlighted as a valid source of insight about detransitioning across the board.

Lastly, in short, researchers in Spain in 2023 published a “critical review of the literature” about detransitioning. They found that estimates of regret-based detransitioning ranged from zero to 13.1%. Discontinuation of cross-sex hormone treatment ranged from 1.9% to 29.8%. This included zero to 2.4% of those who detransitioned with regret after surgery and zero to 9.8% who did so after cross-sex hormone treatment.
“The politicization of the phenomenon” of detransitioning, the authors wrote as their final word in their paper, “creates an atmosphere of censorship that affects people who detransition, people undergoing gender transition processes, and the professionals involved.”
I am an independent journalist, specializing in science and health care coverage. I contribute to The New York Times, The Guardian, NBC News and The New York Sun. I have also written for the Washington Post, The Atlantic and The Nation. Follow me on Twitter: @benryanwriter. Visit my website: benryan.net
It's really important to assess the prevalence of detransition, but that should not overshadow the importance of the prevalence of desistance, those who change their minds before they begin medicalizing.
Parents especially benefit from knowing that watchful waiting instead of impulsive action usually ends up being the wisest course. It certainly was for us; our 11-year-old desisted from her non-binary identification on her own after 2.5 years of us not making a big deal of it or acting on any rash recommendations.
This 2021 US/Canadian study showed that the desistance rate among boys first diagnosed before puberty was 88% by late puberty:
https://pmc.ncbi.nlm.nih.gov/articles/PMC8039393/
This 2024 German study showed that desistance rates in the 15-24 age group ranged from 50% to 73% after 5 years:
https://ourduty.group/2024/06/11/german-study-desistance-is-common/?s=09
A newer study from Norway provides a higher quality analysis from 2000-2023 among minors:
https://pubmed.ncbi.nlm.nih.gov/39648282/