

Youth Gender-Transition Treatment Not Tied to Lower Suicide Deaths in Finland
Youth Gender-Transition Treatment Not Tied to Lower Suicide Deaths in Finland
Such treatment for adolescents with gender dysphoria was also not linked to lower psychiatric treatment needs, according to preliminary findings from an analysis of Finnish health data.

Among young people with gender dysphoria, medical gender-transition treatment is not associated with a lower rate of death by suicide or less demand for psychiatric treatment, according to preliminary findings from an analysis of decades of Finnish health data.
LGBTQ youths in general and children with gender dysphoria in particular experience a high rate of suicidality, including suicidal thoughts and attempts, according to multiple studies.
A 2021 editorial in The Lancet Child & Adolescent Health criticized efforts in U.S. states to ban gender-transition treatment for children, stating of puberty blockers, “Removing these treatments is to deny life.” Similarly, LGBTQ advocacy groups often state that treating gender dysphoria among children and adolescents with puberty blockers and cross-sex hormones is “life saving.”
The new findings from Finland, which have not yet been published or subjected to peer review and therefore should be interpreted with caution, contradict that claim.

Researchers examine the rising tide of gender distress in global youth
Dr. Riittakerttu Kaltiala, a professor of adolescent psychiatry and the chief psychiatrist at Tampere University Hospital in Finland, presented preliminary findings from her team’s study of data regarding gender dysphoric youth at the Society for Evidence Based Gender Medicine’s (SEGM) conference this week in New York City.
SEGM is a coalition of clinicians and researchers who share concerns about what the group characterizes as a “lack of quality evidence for the use of hormonal and surgical interventions as first-line treatment for young people with gender dysphoria.” The conference was attended by about 75 people, including academics, physicians, mental health professionals, lawyers, parent advocates and journalists. They heard from an array of speakers who examined the scientific evidence concerning the care and treatment of gender dysphoric youths.
SEGM is controversial, derided by transgender activists as a fringe group whose ideas, they assert, are hostile to transgender people’s autonomy and well-being. Conference attendees were asked to keep secret the event’s location. Security guards were on site.
During the aughts, Finland was among the first nations to adopt what is known as the “Dutch protocol” for treating gender dysphoria in minors with puberty blockers and cross-sex hormones. Like many other nations, Finland has seen a sharp rise in recent years in gender dysphoria diagnoses in young people. A disproportionate share of these youths were designated as female on their original birth certificate.
Finland, Sweden and England’s health authorities ultimately conducted systematic reviews of the scientific evidence supporting such medical treatment of gender dysphoria in children. The reviews found the evidence was of low quality or otherwise inconclusive. Consequently, these three nations, along with Norway, have sharply reduced the availability of puberty blockers and cross-sex hormones for gender dysphoric youths. Instead, they have established psychological counseling as first-line treatment for this vulnerable population.

The relevant legal landscape has fractured in the United States, with over 20 state legislatures passing bans of gender-transition treatment for children. Lacking a central health authority on par with the European nations, U.S. physicians instead look to clinical guidelines for caring for gender dysphoric children from medical societies, notably the Endocrine Society and the trans-medical group WPATH. In 2018, the American Academy of Pediatrics endorsed what’s known as the gender-affirming care treatment model. In August, the AAP reaffirmed that support while announcing it will commission a systematic review of the related scientific evidence.
The new Finnish study
At the SEGM conference, Dr. Kaltiala, who is considered the top expert on youth gender medicine in Finland, asked attendees not to photograph her slides regarding her new study of Finnish youth. She said that the figures remain subject to change. Otherwise, the conference was considered on the record.

Dr. Kaltiala’s team examined data from Finland’s health registry, which provided what she characterized as excellent national data. (Nordic nations are famous for such rich, centralized health-data sources.) They identified nearly 2,100 adolescents who were diagnosed with gender dysphoria under the age of 23 since the 1990s. The team established a group of 17,000 matched-control individuals. There was an average of nearly seven years of follow-up data on these young people, and a maximum of about a quarter century of follow-up.
The proportion of gender dysphoric youth who were designated as female rose from 14% between 1996 and 2000 to 68% between 2016 and 2019. During this time, adolescents were diagnosed with gender dysphoria at progressively younger ages.
Among the gender dysphoric adolescents, the proportion who had received psychiatric treatment prior to their diagnosis increased from 17% between 1996 and 2010 to 36% between 2011 to 2019. During both time periods, about two-thirds of these young people received psychiatric treatment after their gender dysphoria diagnosis. Among the control group, these indicators of mental health did no change significantly over time.
Dr. Kaltiala and her colleagues wanted to know whether receiving what she called “gender-reassignment” treatment—puberty blockers and cross-sex hormones—was associated with differences in psychiatric outcomes. She did not, however, report how many youths actually received such treatment.
As important background, her team found that among the gender dysphoric youth, those who did not receive gender-reassignment treatment were three times more likely to have received a specialized level of psychiatric treatment prior to their gender dysphoria diagnosis. Additionally, having received a specialized level of psychiatric care was associated with a three-fold greater likelihood of subsequently receiving psychiatric care among gender dysphoric youths.
When the investigators controlled the data for prior psychiatric treatment, registered sex and birth year, they found that compared with the control group, the gender dysphoric youths had a higher likelihood—about 3.6-fold to 3.9-fold higher—of later receiving psychiatric care, one that held regardless of whether they received gender reassignment treatment.
“Medical gender reassignment was not protective of subsequent psychiatric treatment needs,” Dr. Kaltiala said.
The suicide data
Dr. Kaltiala next addressed the crucial question of whether gender transition treatment is associated with a lower likelihood of death by suicide.
As context, she referred to a 2022 paper by Michael Biggs, a sociologist at the University of Oxford, who was also at the SEGM conference. Published in the Archives of Sexual Behavior, Biggs’ analysis examined 2010 to 2020 data regarding some 15,000 gender dysphoric children and adolescents younger than 18 in England, Wales and Northern Ireland who were cared for by the Gender Identity Development Service (GIDS) at the Tavistock clinic. There were data covering approximately 30,000 cumulative years spent in the GIDS program, including on the waiting list, by these young people.
During this time, four of these young people were known or suspected to have died by suicide, two of whom were on GIDS’s waiting list and two who were receiving care. (Biggs told me that his analysis was unlikely to have missed any deaths because of U.K. National Health Service reporting requirements for deaths.) This translated to an overall suicide death rate of 13 per 100,000 gender dysphoric youths—a rate approximately 5.5 times higher than other youths. (Biggs did not compare this suicide death rate to youths who had a rate of psychiatric diagnoses as high as seen in the GIDS patients.)
Also at the SEGM conference was British journalist Hannah Barnes, whose book, “Time to Think: The Inside Story of the Collapse of the Tavistock’s Gender Service for Children,” chronicled the tumultuous and controversial history of the GIDS program.

In the Finnish cohort, seven, or 0.3%, of the gender dysphoric adolescents died by suicide, compared with 20, or 0.1%, of the matched control group. This meant a suicide death rate per 100,000 cumulative years of follow-up of 51 gender dysphoric youths and 12 control-group young people. This difference was statistically significant, meaning it is unlikely to have been driven by chance.
When the researchers controlled the data for birth year, registered sex and psychiatric diagnoses, they found that receiving gender-reassignment treatment was not associated with a significant difference in the rate of death by suicide.
Dr. Kaltiala and her colleagues concluded that the prescription of puberty blockers and cross-sex hormones was not associated with any difference in psychiatric outcomes, including the chance of death by suicide. Gender dysphoric youth had a higher rate of psychiatric conditions than their peers to begin with; and it was those conditions that predicted further psychiatric care needs and death by suicide.
“Medical gender reassignment does not resolve or diminish the risk for severe psychiatric morbidity,” Dr. Kaltiala said.
She stressed that suicide deaths among gender dysphoric youths in Finland were “very rare”.
Further exploration of the suicide issue
The SEGM conference also heard a presentation from Dr. Alison Clayton, a consultant psychiatrist and specialist psychotherapist and a PhD candidate at the University of Melbourne’s School of History and Philosophy of Science, on the scientific knowledge base regarding suicide risk among gender dysphoric youth and the question of whether puberty blockers and cross-sex hormones reduce this risk.
As Emily Bazelon reported in The New York Times Magazine in 2022, parents of gender dysphoric children have reported that they often hear the mantra, “It’s better to have a live son than a dead daughter.” This suggests that the likelihood of death by suicide among gender dysphoric youths is substantial and can be substantially mitigated through gender-transition treatment
Dr. Clayton characterized this mantra as coercive for families weighing the risks vs. benefits of gender-transition treatment for children. After hearing such a statement, she said, “What parent is going to be able to look at the evidence and be in a position to evaluate that evidence?”
Her analysis of the relevant scientific literature complemented the Finnish findings. Dr. Clayton said that there is no reliable evidence that gender-transition treatment decreases suicidality or mortality. She pointed to the United Kingdom’s systematic review of such treatment, which found that all the relevant studies examining the suicidality question were of poor quality and provided low-certainty evidence. She criticized studies that have suggested such treatment prevents suicidality, saying they “trumpet findings, but hide the limitations behind the paywall.”
While Dr. Clayton did not refer to this particular paper, it’s valuable to examine a study published in 2022 by Diana Tordoff, an epidemiologist at the University of Washington, in JAMA Network Open. This observational cohort study concerned 104 transgender, nonbinary or gender-fluid youths age 13 to 20, 7% of whom were on gender-transition treatment at the study’s outset. After 12 months, two thirds had started puberty blockers, cross-sex hormones or both.
This study’s top-line findings have been widely publicized: that gender-transition treatment was associated with a 60% lower odds of depression and a 73% lower odds of suicidality among young people. The fact that this study was not a randomized controlled trial notwithstanding, a press release from the University of Washington used causal language to characterize its findings, stating, “Gender-affirming care can improve mental health outcomes in transgender youth.”
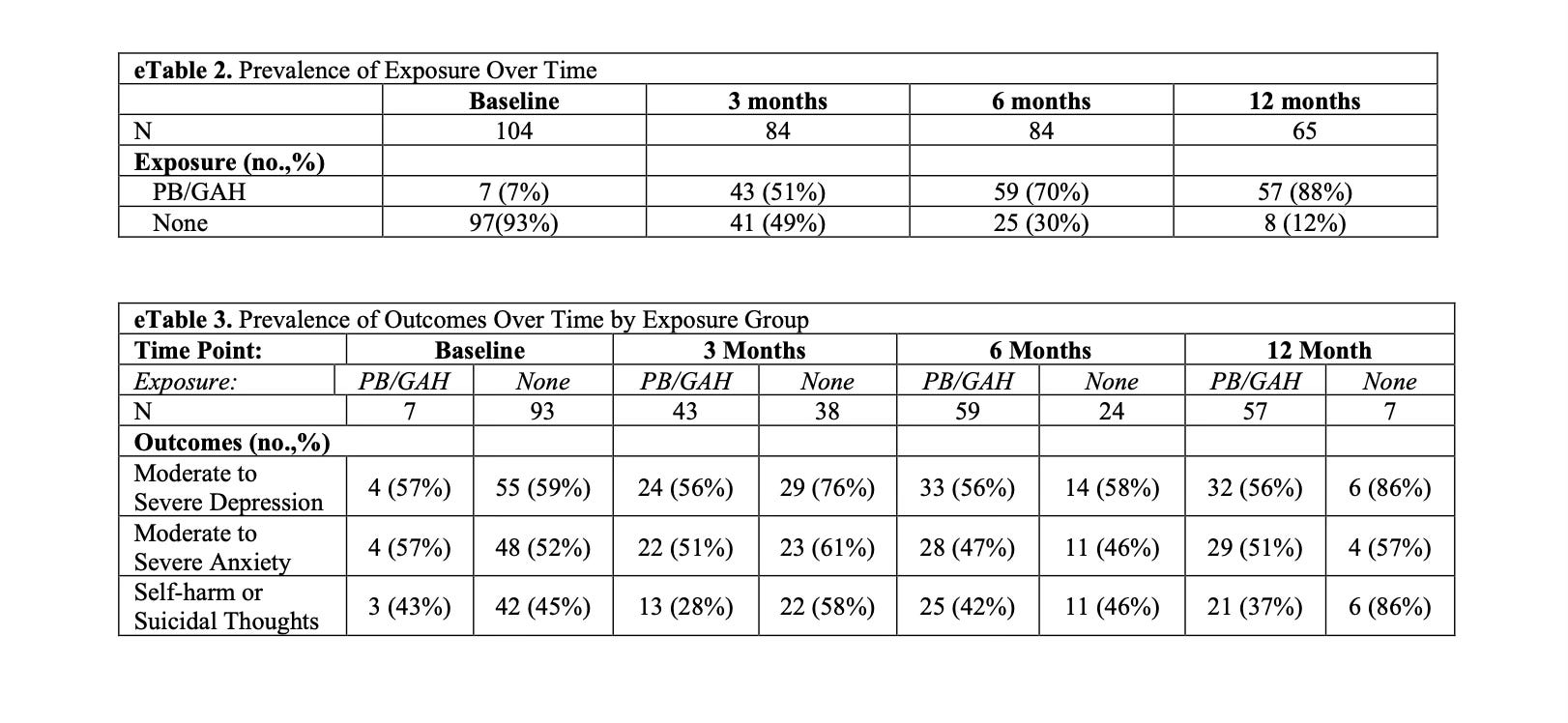
But a closer look at the data shows that between the study’s outset and the 12-month mark, the depression and suicidality scores did not change significantly among the young people who received gender-transition treatment. The study’s key findings were derived from a comparison between this group and the still-untreated group’s mental-health metrics at the study’s baseline and months 3, 6 and 12. But the study saw a disproportionately high drop-out rate among untreated individuals, with only six of the 35 remaining untreated youths completing the final mental health questionnaire; and this group was especially psychologically unwell. It remains unknown how the study’s findings might have been different had all 35 of the untreated participants reported all of their mental health metrics.
Dr. Clayton did scrutinize the January 2023 New England Journal of Medicine paper examining outcomes among 315 transgender and nonbinary youths, age 12 to 20, who were treated with cross-sex hormones and followed for two years. She criticized the paper for providing “no extra detail or discussion of the significance [or] meaning” of the fact that two of these participants, or 0.6%, died by suicide.
In her final slide, Dr. Clayton expressed a litany of concerns about the prevailing rhetoric regarding suicide risk among transgender and gender-diverse (TGD) youths, stating, “The current suicide narrative around TGD young people may increase risk of suicidality and suicide in vulnerable young people.”
Referring to gender-affirmative treatment (GAT), she continued: “Making strong claims regarding GAT decreasing suicidality/suicide risk which are unsupported by the evidence places an unfair burden on parents and may be coercive, thus undermining the informed consent process. Suicide risk should not be exaggerated or inappropriately used to manipulate parents and young people into agreeing to gender-affirming treatments.”
*****
For a much more detailed—and frankly scathing—analysis of the apparent shortcomings in Tordof et al’s analysis, check out Jesse Singal’s Substack on the matter.
Please Share this Substack on Twitter by retweeting my tweet. If you’re of the mind to, kindly comment on this article both here on Substack and on Twitter.
This reads like the cliff notes of pediatric gender affirming care of a very difficult college course, called “What’s Does the Science Say? : A takedown of pediatric gender medicine”. You brought up my top favorite worst studies EVER:
Tordoff study with a control group of ...7!
NEJM leaves out two scales AND has 2 completed suicides, they still have the audacity to publish they found mental improvement!
Benjamin you are a investigative reporter...where in the world are the 6 missing scale results?” You’d win a Pulitzer if you find them...find them. Don’t you know some people in high places? I want to see you on 60 Minutes discussing this scandal with the Coop.
How did you manage to report on this conference, make it coherent, add links from studies and write such a concise synopsis in a way that that readers will certainly learn some or many new insights on this topic?...well this deserves to be published the NYTS or the Atlantic.
Other than leaving out the ketchup placebo idea...you nailed it.
I have a question for you. Why do you think SEGM is considered to be a controversial organization, and do you have an opinion on SEGM?
thank you for your analysis and clear writing.